Defending Women and Transgender Persons Facing Extreme Sentences: A Practical Guide
“Using capital punishment or incarceration as the sole response to violence fails to achieve justice for all because you’re simply sending people, especially black and brown people, into a system that has already failed them.” —Erica Sheppard, incarcerated on death row in Texas, U.S.
| COVER PHOTOGRAPH: Marie Dawandala, Damaris Doukouya, and Martha Weteya on October 23, 2020, the day they left prison as free women after spending over 5 years behind bars. Before a court overturned their sentence, the three Cameroonian women had been sentenced to death under Cameroon’s draconian anti-terrorism laws. The Cornell Center on the Death Penalty Worldwide advocated on their behalf as part of an international defense team led by Me. Nestor Toko. |
Table of Contents
Introduction: Why Do We Need Special Skills to Defend Women?. 2
Gender Identity and Expression. 5
Chapter 1: Building a Gender-Sensitive Team. 8
Gender-Sensitive and Inclusive Team Dynamics. 8
Chapter 2: Conditions of Detention for Women Facing Extreme Sentences: What You Need to Know 11
The International Legal Framework for Women in Detention. 11
The Right to Family Contact 11
Housing and Solitary Confinement 13
The Right to Adequate Medical and Mental Health Care. 13
Transgender and Non-Binary Prisoners. 14
Violence in Prisons and Police Stations. 15
Chapter 3: Women and Mental Health: Considerations for Defense Teams. 17
Postpartum Mental Disorders. 24
Gender Differences for Serious Mental Illness. 25
Chapter 4: Gender-Based Violence: Myths and Misperceptions. 27
Understanding Gender-Based Violence. 27
Sexual Violence: Myths and Misperceptions. 30
Domestic Violence: Myths and Misperceptions. 34
Interviewing Your Client About Gender-Based Violence. 37
Chapter 5: Treatment of Women in the Criminal Legal System.. 48
Women and Police Interrogations. 48
Bias from Judges and Prosecutors. 49
Women with Male Co-Defendants. 50
Intersectional Discrimination. 51
Chapter 6: International Human Rights Law.. 54
Human Rights Law and Women’s Death Sentences. 54
Using Human Rights Law to Reframe the Narrative. 55
Chapter 7: Working With the Media. 59
Media Coverage of Women Defendants. 59
How to Work with the Media. 59
Chapter 8: Further Reading.. 61
Chapter 2: Conditions in Jails and Prisons. 61
Chapter 3: Women and Mental Health. 61
Chapter 4: Gender-Based Violence. 62
Chapter 5: Treatment of Women in the Criminal Legal System. 62
Chapter 6: International Human Rights Law. 63
Chapter 7: Working with the Media. 64
Gender-Sensitive Client Interview Form. 66
Acknowledgements
The principal authors of this guide were Sandra Babcock, Nathalie Greenfield, Gabriela Markolovic, and Jessica Sutton. Joshua Howard and Adrienne Larimer also authored key sections of the guide. We would like to extend a special thanks to our excellent team of editors and proofreaders, including Maci East, Hailey Shapiro, Alexandria Kim, Seoyeon Shin, and Sabrina Bryan. We also would like to thank Katie Vaz for her assistance in designing the report. The authors are immensely grateful to the women and transgender persons who shared their stories with us. We would like to recognize, in particular, Kwaneta Harris, Christa Pike, and Erica Sheppard, whose reflections on their experiences of incarceration have enriched this manual. We are in awe of their strength, and we stand in solidarity with those who remain incarcerated in legal systems that failed them in so many ways. We would also like to thank the Human Rights Initiative at the Open Society Foundations, whose support made this report possible. We are particularly grateful to Louise Ehlers of OSF. Louise has been a wonderful partner over the last two years, and she has been a champion of our work around gender and the death penalty from the very beginning. The Cornell Center on the Death Penalty Worldwide takes sole responsibility for the final content of the report.
Introduction: Why Do We Need Special Skills to
Defend Women?
The overwhelming majority of lawyers have never received any special training on how to defend women facing extreme sentences. Most of us simply approach the cases of women as we would any other male client. Yet the cases of women invariably require specialized knowledge and skills that most lawyers lack. And because we don’t know what we don’t know, lawyers around the world routinely misinterpret critical evidence and fail to uncover facts that are essential to effectively defend women. This guide is a first attempt to remedy our collective ignorance. We begin with the basics: how to create a gender-sensitive team and build relationships of trust with your women clients. We provide a glossary of terms so that you have a gender-sensitive vocabulary. Significantly, when we discuss “women” in this manual, we include both cis women and transgender persons, as well as other non-male members of the LGBTQ+ community. In Chapter 2, we describe how conditions in jails and prisons often fail to protect women’s basic human rights. This chapter includes a section devoted to the rights of transgender prisoners, who are frequently deprived of essential medical treatment and suffer cruel and dehumanizing conditions of confinement. Armed with this knowledge, you can learn what questions to ask your women clients about their experiences in prison so that you can better protect their rights. Chapter 3 addresses mental health issues that are commonly found in cases of women. Every lawyer defending a client accused of a capital crime should have a strong grasp of the causes and symptoms of trauma; this is especially true when defending a woman. The great majority of women facing extreme sentences have experienced gender-based violence and a wide range of adverse childhood experiences. These experiences invariably lead to trauma, which can cause debilitating, lifelong mental distress. Trauma shapes your client’s life trajectory before she even enters the criminal legal system. It can also affect how she responds to police interrogators, how judges and juries perceive her behavior, and how she interacts with her legal team. Chapter 3 also provides an overview of Post-Partum Depression, a mental illness that often affects women who kill children. Finally, Chapter 3 discusses how the symptomology and onset of common mental illnesses differ between men and women. In Chapter 4, we address the epidemic of gender-based violence, which touches nearly all of our clients’ lives. We touch on some of the major myths and misperceptions about the behavior of women who are in violent relationships. We also provide guidance for discussing this topic with your clients. We live in a global culture where violence against women is widely tolerated and normalized. As a result, lawyers risk minimizing the consequences of sexual and other forms of violence against women. Frequently, lawyers fail even to ask their clients about their experiences of gender-based violence, perhaps because the topic is a sensitive one. One of the lessons we seek to convey is the importance of talking about sex—and ensuring that you have someone on your team who is comfortable engaging in these conversations with your client. Chapter 5 provides an overview of how women are treated in the criminal legal system. Women can be particularly vulnerable to aggressive police interrogation, and may be subjected to sexual threats or violence in police stations and jails. Their experiences of trauma can also make them more suggestible and more likely to admit guilt. At trial, prosecutors frequently seek to de-feminize women as a way of encouraging judges and juries to condemn their behavior. In addition, prosecutors often minimize their experiences of gender-based violence to discredit them. Prosecutors also rely on negative gender stereotypes, sometimes casting women as hyper-sexual, other times criticizing their mothering skills, in an effort to encourage harsh punishment. Defense teams must anticipate these tactics and take steps to prevent them—or at the very least, object when prosecutors utilize them. In this chapter we also highlight the myriad of ways that women can experience discrimination on the basis of multiple identities. Understanding these intersecting forms of discrimination is vital when defending women who are members of minority groups, foreign nationals, disabled, or gender-non-conforming. Finally, we discuss the risks women face when they are prosecuted alongside male co-defendants, and the importance of obtaining separate counsel for each defendant. The international legal framework for understanding the rights of women is addressed in Chapter 6. International human rights treaties, and their interpretation by courts and experts around the world, establish that governments have an obligation to protect women from gender-based violence and other violations of women’s human rights. In many, if not most cases of women facing extreme sentences, the state will have violated these obligations. Understanding that the government has failed in its responsibility to protect your client’s rights helps to shift the narrative of your case from one that attributes blame exclusively to your client, to one that acknowledges that the state bears some responsibility for the conditions that gave rise to her behavior. Finally, we address the role of the media in women’s cases and provide guidance on working with the media in Chapter 7. We conclude by providing a bibliography of further reading. This guide provides an overview of key topics in the defense of women, but it is by no means exhaustive. This manual is best read in tandem with two separate publications by the Cornell Center on the Death Penalty Worldwide, both of which are available online: Judged for More Than Her Crime, a global report on women facing the death penalty (https://deathpenaltyworldwide.org/publication/judged-more-than-her-crime/); and Representing Individuals Facing the Death Penalty: A Best Practices Manual (https://deathpenaltyworldwide.org/publication/representing-individuals-facing-the-death-penalty-a-best-practices-manual/). The Cornell Center on the Death Penalty Worldwide also maintains an online bibliography of helpful references that we continually update. We also keep a library of sample briefs and other litigation documents relating to the defense of women. You can access these materials by emailing [email protected].
We hope this guide is helpful, and welcome your comments and suggestions forimprovement.
Introductory Language
Gender and Sex
Gender: Gender consists of socially constructed roles, behaviors, attributes, and other characteristics that a given society considers appropriate. Because gender is a social construct, gender varies from society to society and can change over time. Gender is also multidimensional and intersects other social categories and identities such as race, ethnicity, class, ability, age, and religion. Gender is frequently viewed as a binary concept of male/female, but many individuals, communities, and societies identify with more than two genders and/or view gender as a spectrum of expression. Gender interacts with, but is different from, biological sex.[1] Gender stereotype: A widely held, simplified, or essentialist belief about a group based on their perceived gender. It manifests as a set of characteristics, preferences, and roles that society not only associates with masculinity and femininity but also imposes as a normative expectation. Sex assigned at birth: A term referring to anatomical, physiological, genetic, or physical attributes. It is typically categorized as male, female, or intersex. There are a number of indicators typically used in determining sex assigned at birth encompassing both primary and secondary sex characteristics, including external genitalia, internal reproductive organs, gonads, hormone levels, hormone receptors, chromosomes, and genes.[2] Intersex: Intersex is a term that refers to people who are born with physical or biological sex characteristics (including sexual anatomy, reproductive organs, and/or chromosomal patterns) that do not fit the typical and/or medical definitions of male or female. The term intersex reflects the biological variation of sex. For example, a person may be born with mosaic genetics, so that some of their cells have XX chromosomes and some of them have XY. Others may have external female-typical anatomy but have mostly male-typical anatomy internally. This can be through variations in hormones, chromosomes, internal or external genitalia, or any combination of any or all primary and/or secondary sex characteristics. Many intersex people are noticed as intersex at birth, but many others are not and do not discover this until adolescence or adulthood. As intersex is about biological sex, it is distinct from gender identity and sexual orientation. Historical medical terms such as hermaphrodite are no longer acceptable or accurate and should not be used.
Sexual Orientation
Sexual orientation: A person’s romantic, sexual, and/or emotional attraction to another person. LGBTQ+: An acronym referring to Lesbian, Gay, Bisexual, Transgender, and Queer individuals and/or communities. The “plus” sign includes other identities, such as pansexual or two-spirit. You may also see LGBTQIA, which includes Intersex and Asexual/Ally. Both acronyms are inclusive and acceptable, although some organizations may prefer one over the other. Lesbian: A term referring to a woman who is emotionally, romantically, and/or physically attracted to other women. Gay: A term used to describe people who are emotionally, romantically, and/or sexually attracted to people of the same sex and/or gender. A person may identify as gay even though that person does not have any sexual experience or any sexual experience with a person of the same gender and/or sex. A person may identify as gay despite having previously identified as straight or heterosexual and/or having relationships with individuals of the opposite sex and/or gender. Bisexual: A term referring to a person who is emotionally, romantically, and/or sexually attracted to people of more than one gender, though not necessarily at the same time, in the same way, or to the same degree. Queer: An umbrella term used by some LGBTQ+ people to describe a sexual orientation, gender identity, or gender expression that does not conform to dominant social norms. Queer is not only used as a self-identification but may also be used to describe communities. Historically, the word “queer” constituted a negative or pejorative term for people who are LGBTQ+, and some individuals may find the word offensive.
Gender Identity and Expression
Gender identity: A person’s deeply felt, core sense of self in relation to gender (see Gender). Gender identity may or may not correspond to sex assigned at birth or to a person’s primary or secondary sex characteristics. Because gender identity is internal, a person’s gender identity may not be visible to others, and it is determined by self-identification. People become aware of their gender identity at many different stages of life, from childhood to adulthood, and a person may disclose their gender identity at different times and to some people, but not others. Gender identity is a separate concept from sexuality (see Sexual Orientation) and gender expression (see Gender expression).[3] Gender expression: The manner in which a person communicates gender to others within a given culture, such as clothing, appearance, or mannerisms. All people have gender expression. This communication may or may not reflect a person’s gender identity or sexual orientation. While many people’s gender expression relates to social constructions of masculinity and femininity, there are countless combinations that may incorporate both masculine and feminine expressions —or neither (e.g., androgynous expressions).[4] Cisgender (pronounced sis-gender): A term used to refer to an individual whose gender identity aligns with sex assigned as birth. Transgender: An umbrella term describing the wide range of people whose gender identity and/or gender expression does not necessarily conform to their assigned sex at birth. Transgender people may or may not decide to transition socially or medically. Because transgender is an umbrella term, the term may refer to, but is not limited to, people who identify as transsexual, non-binary (identifying not exclusively as male or female), genderqueer, or gender nonconforming. See below for common acronyms and terms including female to male (or FTM), male to female (or MTF). Non-Binary: An umbrella term encompassing gender identities and expressions existing outside of the binary definitions of man or woman, masculine or feminine. Gender nonconforming: A self-identifying term used by some people to describe gender identities and expressions that do not adhere to the gender norms and roles commonly associated with sex assigned at birth. Related but not equivalent identities include gender-expansive, genderfluid, and genderqueer. Two-Spirit: A term used within some Native American and Indigenous communities to refer to a person who identifies as having both a male and a female essence or spirit. In some Native American and Indigenous communities, two-spirit people traditionally occupied a distinct, alternative gender status(es) and in some tribes constituted a third or fourth gender. Notably, there are hundreds of distinct Native American and Indigenous communities that encompass varying gender identities, expressions, and roles; there is no universal experience or culture and no universally used or accepted term. Non-indigenous people should not use this term.
Transition
Transition: A term used to describe the process that a person undergoes to affirm a gender identity that is different from sex assigned at birth. This process may be a social transition, such as using new names, pronouns, or clothing; it may be a legal transition, such as legally changing one’s name or gender markers on documents; it may be a medical transition, such as taking hormones or undergoing gender-affirming surgery. An individual may choose to undergo a combination of these processes, all of them, some but not others, or none at all. There are also financial and institutional hurdles that limit the ability of many people to transition. Many individuals choose not to or are unable to transition for a wide range of reasons both within and beyond their control. Importantly, the validity of an individual’s gender identity does not depend on any social, legal, and/or medical transition; the self-identification itself is what validates the gender identity. Deadnaming: This occurs when an individual uses the birth name of a transgender or non-binary person who has changed their name as part of their gender transition. This may result in trauma, stress, embarrassment, and even danger. Gender dysphoria: A concept designated in the DSM-5[5] as clinically significant distress or impairment related to a strong desire to be of another gender, which may include the desire to change primary and/or secondary sex characteristics. Not all transgender, non-binary, or gender nonconforming individuals feel gender dysphoria. Some jurisdictions, agencies, institutions, and/or practitioners require a diagnosis of gender dysphoria before providing gender-affirming services, such as gender-affirming health care and housing. Gender-affirming health care: Health care that holistically attends to a transgender or non-binary person’s physical, mental, and social health needs and affirms that person’s gender identity. Gender-affirming surgery: Surgical procedures that can help people adjust their bodies to more closely match their innate gender identity. Not every transgender or non-binary person will desire or have resources for gender-affirming surgery, and surgery does not define one’s gender identity. Use this term in place of the older term “sex change.” Hormone Replacement Therapy (HRT): A type of gender-affirming treatment that allows transgender and non-binary people to medically transition or feel more at home in their bodies (see Gender-Affirming Surgery and Transition). Those taking testosterone (masculinizing hormones) may grow more facial/body hair and notice their voices deepening. Those taking estrogen (feminizing hormones) may experience a redistribution of weight, breast development, and a decrease in body hair. Bottom surgery: Surgery performed on an individual’s reproductive system as a part of gender-affirming surgery. (See Gender-Affirming Surgery.) Transgender and non-binary individuals may or may not have the desire or resources to pursue bottom surgery. As with any other aspect of transition, trans people retain the right not to discuss their surgical history, and surgery does not define gender. Top surgery: Surgery performed on an individual’s chest/breasts as a part of gender-affirming surgery. (See Gender-Affirming Surgery.) For some individuals who were assigned female at birth, top surgery may encompass a chest reduction or full removal. For some individuals who were assigned male at birth, this can be an increase in chest size using saline or silicone. Transgender and non-binary individuals may or may not have the desire or resources to pursue top surgery. FTM/F2M: An abbreviation of Female to Male; a transgender man. MTF/M2F: An abbreviation of Male to Female; a transgender woman.
Other Terms
Chosen family: Individuals who support an LGBTQ+ person, who are not biologically related, and who may fill the role of that person’s biological family if an LGBTQ+ person’s family is not supportive. Gender-sensitive: Strategies, plans, and policies that recognize gender-based differences and aim to eliminate gender inequality. Gender-based violence: Violence directed towards a person based on their assigned sex at birth or gender identity and expression and grounded in unequal power relationships. It encompasses physical, sexual, verbal, emotional, and economic harm, including threats and coercion. It should not be conflated with “violence against women,” which excludes a broad understanding of gender. Homophobia: Interpersonal or institutional discrimination, bias, violence, or other negative attitudes or behaviors towards LGBTQ+ people due to their gender identities and/or sexual orientation. Intersectionality: The complex and cumulative effect of discrimination resulting from the combination of different marginalized forms of identity. Intersectionality theory is rooted in the work of U.S. Black feminist scholarship; the term “intersectionality” was originally coined by Kimberlé Crenshaw, who, when writing about the forms of legal discrimination that African American women experience, explains: “Because of their intersectional identity as both women and of color within discourses that are shaped to respond to one or the other, women of color are marginalized within both.” Other feminists have taken a broader approach to the concept of intersectionality. June Eric-Udorie, for example, argues that “[i]ntersectionality offers us a way to understand how multiple structures—capitalism, heterosexism, patriarchy, white supremacy, and so on—work together to harm women who are poor, disabled, queer, Muslim, undocumented, not white, or a combination of those things. Intersectionality is a way for marginalized women to talk about how their lives are affected by multiple oppressive structures…” Intersectionality theory highlights that a person’s identity may compose of a multitude of marginalized identity markers, such as gender, race, ethnicity, sexuality, disability, religion, or class, to name a few. Transphobia: Interpersonal or institutional discrimination, bias, violence, or other negative attitudes or behaviors towards transgender, gender nonconforming, and non-binary people due to their gender identities and/or expressions.
Chapter 1: Building a Gender-Sensitive Team
Many of you reading this manual may be representing your very first woman facing capital punishment or another extreme sentence. In this chapter, we will explain why it is critical for you to provide legal representation that is both culturally competent and gender sensitive. Put differently, you and other members of your team must understand the ways in which a client’s gender identity affects her experience within the criminal legal system. Women (including cis women, trans women, and non-binary women) are subject to gender bias throughout their lives, including in their interactions with the criminal justice system. Gender affects their interactions with law enforcement, perceptions of the judge and/or jury, prosecutorial narratives, communications with the defense team; family obligations and dynamics; conditions of confinement; and potential for reentry.[6] A defense team must also be aware of how a female client’s gender identity and expression has affected her life experiences, including, but not limited to the following:
- Family dynamics
- Discipline by caregivers
- Education
- Sexual development
- Romantic and sexual relationships
- Employment
- Class, wealth, and income
- Military experience
- Physical health
- Mental health
- Pregnancy
- Gender-based interpersonal violence
- Gender-based institutional and state violence[7]
The above areas are not exhaustive, as gender affects all areas of life. Ultimately, understanding the role of gender in a client’s life experiences is critical to developing the narrative of a client’s life and conveying that story in a culturally competent way that resonates with the decision-making body. If you work in a jurisdiction where more than one lawyer is appointed to represent indigent clients, you should ensure that at least one member of the team is a woman. Being female is not synonymous with providing gender-sensitive and culturally-competent legal representation, but clients may be more comfortable disclosing certain facts to a female member of the team. This is why the United Nations Principles and Guidelines on Access to Legal Aid in Criminal Justice Systems provide that States should take “active steps to ensure that, where possible, female lawyers are available to represent female defendants.”[8] In addition, you should ensure that you seek assistance from gender-sensitive experts, investigators, paralegals, and others. Later in this guide, we provide specific suggestions for how you can sensitively interview your client. If you are a sole practitioner (of any gender) and the court will not appoint more than one lawyer to defend your client, you can still provide gender-sensitive legal representation, but you will need to know your limitations and take steps to overcome them. In particular, you should: (1) recognize the areas in which you lack expertise, education, or awareness; (2) seek support, consultation, and assistance from professionals in associated fields, such as mental health, who possess specific cultural knowledge and expertise; and (3) educate yourself and the court about the ways in which gender has shaped a client’s experiences.
Gender-Sensitive and Inclusive Team Dynamics
In addition to considering the role of gender in shaping your client’s historical and contemporaneous experiences, a defense team must also be sensitive to the role of gender identity and expression in team dynamics and client relationships. This requires self-awareness, open-mindedness, resistance to stereotyping, and a willingness to reconsider views that you have developed from your upbringing and culture. Defense team members may have internal gender bias that hinders the development of trust and rapport with the client, effective communication within the team, and the ability of a client to assist in her defense. Gender bias can cause people to interrupt a female client or female team member; dismiss or invalidate a client’s lived experiences, concerns, or reactions; presume that a female client is heterosexual; or rely on socially constructed and restrictive concepts of womanhood or motherhood to value or de-value a female client. Such displays of gender bias can undermine the development of rapport with a client and within a defense team, and can impair your ability to provide effective representation. You must constantly work to achieve self-awareness and accountability and encourage open dialogue within your team (including with your client) to overcome any internal bias that may lead to resentment or mistrust.
Intersectionality
A gender-sensitive defense team must also have an intersectional perspective that takes into account the way a client’s gender identity and expression intersect with that client’s race, ethnicity, nationality, language, class, ability, and sexual orientation, among other identities. In other words, it is not sufficient to evaluate the role of a client’s gender alone, as a female client’s experience as a woman is shaped by other identities as well. For example, the experiences of a wealthy female client in the criminal justice system may differ significantly from those of a poor female client. Both women’s experiences are shaped by gender, but they are also shaped by class. Similarly, a defense team member must examine their own internal bias through that intersectional lens. This bias is pervasive¾in one study of incarcerated LGBTQ+ people in the U.S., over 50% of trans women and nonbinary people reported feeling discriminated against by their defense attorney because of their gender identity and/or sexual orientation.[9] Over 40% of that same group of LGBTQ+ respondents also felt that their attorney discriminated against them on the basis of race.[10]
Meeting the Needs of Transgender Clients Facing the Death Penalty: One Lawyer’s Experience
I knew that getting a new client sentenced to death in the middle of a pandemic was not good. My impressions of the case were not unlike many of my other cases. An indigent person had received counsel who did not have the knowledge, time, or skill to represent their client properly. What made this case different and so shocking, was that my client’s trial lawyers had not even bothered to learn the gender of their client. When I received my assignment, I did what I always did. I looked at the few available documents, looked my new client up in the corrections system, and drafted an introduction letter advising the client that I would be assisting them in their post-conviction appeals. Because it was in the middle of a pandemic, I also apologized to the client for not being able to meet in person. I addressed the letter to “Mr.” John Friendly (not the client’s real name). The response I received back from my client was a friendly, but guarded, hand-written letter. The letter thanked me for letting them know that I would be assisting them, asked a few questions about what that would mean, and asked a little bit about the process. The letter also expressed some skepticism at pursuing the appeals at all. At the end of the letter, the client also advised that she used female pronouns and would like to be addressed by her proper first name, Jane. Finally, the letter thanked me for my time and attention and was signed, Jane Friendly. I immediately wrote back to my client and apologized for my assumption in using a male honorific. I advised that I would, of course, address her by her chosen name and asked if she had any other needs or preferences that she would be comfortable sharing. I addressed her legal questions and sent her the letter, not thinking much about it. The response I received from her was overwhelming. She disclosed that she was shocked by my acceptance and response, and that she had never before received that type of response when advising an attorney that she was female. In the past, she had been dismissed, advised that telling a jury that would be a wrong move, or simply ignored. She was profusely grateful and asked if we could schedule a call to talk. During that initial call, she opened up so much and asked about her appeals and trial. She said that my response to her letter had convinced her that maybe she finally had someone who would fight for her. From there, Jane put her trust in our team, and we haven’t looked back. Jane has told us that our advocacy helped her regain confidence and motivated her to fight for herself, and to want to live again. She has said that the simple act of compassion and kindness when responding to her request to be correctly gendered has stopped her from giving up hope and volunteering for execution. She calls her team of lawyers her real-life miracles.
Chapter 2: Conditions of Detention for Women Facing Extreme Sentences: What You Need to Know [11]
“Even though this prison is technically called a ‘rehabilitative center,’ there is no rehabilitation here, just punishment.” —Christa Pike, incarcerated on death row. National criminal justice systems and prisons are largely designed by men and for men and often overlook women’s specific needs and vulnerabilities. For one thing, the great majority of women in detention are mothers who, before their arrest, cared for children and other family members. At the same time, women facing extreme sentences are often more isolated than men, and receive few family visits. Women in detention are vulnerable to sexual assault by male guards. And women’s medical needs are often ignored. Moreover, LGBTQ+-identified women, transgender, and non-binary persons experience disproportionately high rates of incarceration[12] in large part due to (1) laws that criminalize same-sex relationships, certain sexual acts, and gender non-conforming identities and expressions; (2) pervasive discrimination in housing, employment, health care, immigration, government and social services agencies, and other areas of life; (3) higher rates of poverty, unemployment, and homelessness, and (4) criminalization of survival economies, such as sex work.[13] Once incarcerated, LGBTQ+ women face widespread harassment, bias, and physical and sexual violence as well as unique challenges in the areas of prison rules, disciplinary sanctions, housing, solitary confinement, and medical care.[14] This chapter aims to sensitize defense teams to the particular needs of women facing extreme sentences such as the death penalty. We also provide an overview of the international legal framework that establishes states’ obligations to care for women in detention. Armed with this information, you can inquire after your client’s needs and advocate for humane conditions of detention.
The International Legal Framework for Women in Detention
In 2010, the United Nations Office on Drugs and Crime adopted Rules for the Treatment of Women Prisoners and Non-Custodial Sanctions for Women Offenders (“Bangkok Rules”) to take into account the gender-specific needs of women prisoners.[15] The Bangkok Rules apply a gender lens to an extensive range of issues, providing gender-sensitive guidance on prison admission,[16] security and search procedures,[17] disciplinary procedures,[18] institutional personnel training,[19] and prisoner supervision.[20] The Rules also cover women prisoners’ access to general and female-specific physical and mental health care,[21] training opportunities,[22] and rehabilitation.[23] The Rules stress the importance of women’s communication with family and friends, and especially contact with their children.[24] The Rules also identify considerations for especially vulnerable categories of women: women under arrest or awaiting trial,[25] juvenile female prisoners,[26] foreign nationals,[27] minorities and indigenous women,[28] pregnant women,[29] breastfeeding mothers,[30] and mothers in prison with a child.[31] The 2015 revisions to the United Nations Standard Minimum Rules for the Treatment of Prisoners (“Mandela Rules”) further recognize women’s unique needs. The Mandela Rules have provisions on separated housing,[32] supervision by female prison staff,[33] hygiene,[34] and banning restraints during labor and childbirth.[35] The Mandela Rules also prohibit visiting restrictions as a way to discipline prisoners, particularly women prisoners.[36]
The Right to Family Contact
In many countries, women are the primary caregivers for children and elderly relatives. As a result, restrictions on visitation can be devastating for women prisoners and their dependent family members. Moreover, the social stigma associated with women who are convicted and imprisoned, paired in some cases with restrictive family and child visitation rules, means that many female death row inmates around the world suffer an enduring lack of family contact, contributing to the high levels of depression suffered by women prisoners. Some countries allow female prisoners to bring their young children to prison to live with them. Countries have adopted varying age cut-offs for children in prison; in some prisons children may be allowed to remain with their mothers until the age of three, in others they may remain until the age of seven. In other countries, women are simply not allowed to take their children with them, even if they are breastfeeding. For these women, separation from their children can cause tremendous emotional anguish, particularly if they do not have family members able to care for their children.
Sunny Jacobs: A Mother Wrongly Convicted and Sentenced to Death
The state deprived Sunny Jacobs of her freedom and motherhood. Sunny was breastfeeding her ten-month-old daughter when the police arrested her for a crime that she had not committed. During her detention, she was deprived of all contact with her infant and her nine-year-old son. Sunny continued to lactate, unable to nourish and bond with her baby. She kept thinking that at any moment the state would realize its mistake and reunite her with her children. As time passed, Sunny coped with the loneliness and despair by preparing for her release. Day after day, she collected her milk in a plastic bowl that she secured in the prison, eager to continue to be able to produce milk for her daughter. Without the opportunity to feed her daughter, she sought any way to remain connected with her. For over a year, she drank the milk that she had produced for her baby. The only connections Sunny had to the outside world were occasional letters from family and from her husband, who was also wrongly convicted and sentenced to death. In one letter, she learned that her daughter began to drink milk from a bottle. And her nine-year-old son, who had been held in juvenile detention for over two months, needed psychological help and had to be put in a special school because of the trauma that he suffered at the hands of the authorities. Her despair deepened. Sunny spent seventeen years in prison, five of them while sentenced to death, before she was exonerated. In that time, her parents died, her children entered foster care, and her husband was executed. The foster parents demonized Sunny. They showed her children articles detailing Sunny’s alleged crime, told them they shared her bad DNA, and threatened that they, too, would also end up in prison. When Sunny was released at 45 years old, her children were grown, and she was a grandmother. Sunny now works to educate the public on the death penalty and, with her new husband who was also wrongly convicted and sentenced to death, she heads a foundation to help other wrongly convicted people. She still deals with the trauma of her separation from her children, and the state’s cruel and unjust treatment of her and her former husband. When you are representing a woman who has recently been arrested, she may need your help obtaining information about her children’s welfare. Some lawyers may think that this falls outside the scope of their representation, but if your client is distracted by worry and fear, she will not be able to focus on her legal proceedings. Moreover, showing your concern for your client’s emotional well-being will help build trust and strengthen the attorney-client relationship. Even if your client has no children, she may experience profound isolation from friends and family. Some prisons are geographically isolated or located far from prisoners’ communities, making it expensive and arduous for families to visit.[37] Others, such as prisons in Nigeria or in the United States, maintain strict visitation policies, such as specific days and times that visitors are allowed, increasing the difficulty of planning visits.[38] Many countries allow contact visits; that is, visits where inmates can physically touch their family members and are not separated by a barrier such as glass or bars. There are exceptions, however: some U.S. states deny condemned women all contact visits.[39] In countries where prisoners depend on family members to augment a meager, nutritionally inadequate prison diet, the lack of family visitation can have severe health consequences. While women may bring food to imprisoned male partners or family members, men are less likely to do so—particularly in cultures where cooking is considered to be a woman’s responsibility. Inquiring after your client’s diet and the frequency with which she receives family visits will allow you to gauge her level of social isolation as well as her nutritional needs. Women who identify as LGBTQ+ may experience additional obstacles to visitation as a result of their sexual orientation and/or gender identity and expression. Some individuals may not be in contact with their biological families or may not have biological relatives who can provide financial or emotional support. Some LGBTQ+ persons may have close ties with their chosen family,[40] but most prisons and jails do not recognize these non-biological family members as relatives and have policies that bar or restrict visitation. Similarly, same-sex marriages or long-term relationships may not be recognized and may even be criminalized, which can affect visitation and support. All of these factors can isolate your already-vulnerable LGBTQ+ clients and increase the risk of trauma, suicide, and self-harm.[41]
Housing and Solitary Confinement
One of the most significant obstacles facing LGBTQ+ prisoners, and in particular transgender women, is obtaining safe and gender-appropriate housing in carceral institutions. Most prisons and jails around the world are segregated on the basis of sex assigned at birth and either house male or female prisoners. Therefore, many transgender women are classified by their assigned sex at birth and are housed in male facilities, which disaffirms their gender identity, restricts their ability to express that gender identity through access to gender-affirming clothing, accessories, cosmetics, and hygiene products, heightens their risk of physical and sexual assault by both inmates and staff, and increases their risk of severe psychological distress. While some facilities allow for a trans woman prisoner to transfer to a women’s institution,[42] the majority of carceral institutions globally do not provide for housing classification based on a prisoner’s gender identity. Many institutions acknowledge the increased risk of violence facing trans women in men’s facilities and respond by placing trans women in solitary confinement, purportedly for their own protection. Yet studies show that solitary confinement, which is considered a form of torture by the UN Special Rapporteur on Torture,[43] is often used as a tool of control and violence over transgender women and all LGBTQ+-identified people.[44] Defense teams must therefore understand a client’s housing preference and advocate for LGBTQ+ clients to be safely and appropriately housed, whether that be in a facility that conforms with a client’s gender identity, in protective custody (if that is the client’s preference), in a unit with other LGBTQ+ prisoners, or another alternative. Defense teams should also advocate for gender-affirming clothing, hygiene products, and cosmetics, and challenge policies concerning hair or dress that restrict a client’s expression of gender identity in accordance with a client’s preferences.[45]
The Right to Adequate Medical and Mental Health Care
Male and female prisoners alike receive substandard medical care in most countries. But when prisons fail to provide for women’s unique health needs, they place women at greater risk of infection, illness, or death. At the most basic level, it is challenging or impossible for women to access sanitary pads or other menstruation products in many prisons. In Indonesia, female prisoners must buy pads from the prison commissary store, but these are of poor quality and often lead to discomfort or complications.[46] In other countries, women must make do with alternatives such as newspapers, tissues and pieces of blankets or prison uniforms.[47] “There is no treatment for menopause. Imagine a hot flash in a cell without fans. Climate change means it will be even hotter.” —Kwaneta Harris, currently incarcerated. Access to women’s health services is even more problematic. According to the World Health Organization, “Women are at greater risk than men of entering prison with HIV, hepatitis B and/or hepatitis C.” Incarcerated women are also at higher risk of cervical cancer, yet rarely receive regular screenings.[48] Gynecological and obstetric care is frequently non-existent.[49] In the United States, Thailand and Myanmar, inmates have given birth alone in prison.[50] Women prisoners are also more likely than male prisoners to have severe mental illnesses that remain untreated in detention. They are at higher risk of depression, self-harm, and suicide (see Chapter 3).[51] Knowing this, you should be particularly attuned to your client’s mental and medical health needs. Whenever possible, advocate for your client’s needs by meeting with prison medical staff, prison officers/guards, and wardens.
Transgender and Non-Binary Prisoners
Transgender and non-binary people often face exceptional challenges to receiving gender-affirming health care[52] while incarcerated. Countries that criminalize gender diverse identities and/or expressions almost universally deny gender-affirming health care to prisoners, and even those countries without such criminalization frequently deny adequate health care to transgender prisoners due to pervasive social stigma and marginalization. Of those facilities that provide some form of gender-affirming health care, most require that prisoners have a diagnosis of Gender Dysphoria[53] or a medical history of treatment in order to receive appropriate health care and, even then, many institutions must be forced by court order to provide that care.[54] Gender Dysphoria refers to the feeling of discomfort or distress that might occur in people whose gender identity differs from their sex assigned at birth or sex-related physical characteristics. Those institutions that deny gender-affirming healthcare outright, whether because of cultural stigma, criminalization, or other reasons,[55] create significant risks for the medical and mental health of transgender and non-binary clients. According to World Professional Association for Transgender Health (WPATH), which developed the Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People, “While each patient requires an individualized treatment plan that accounts for the patient’s specific needs, the recommended treatments for people experiencing gender dysphoria include assessment, counseling, and, as appropriate, social transition, hormone therapy, and surgical interventions to bring the body into alignment with the patient’s gender identity.”[56] For prisoners with gender dysphoria, the denial of gender-affirming health care “can result in serious medical issues such as depression, suicidality and self-castration.”[57] In 2017, three trans women in Argentina died “due to complications related to their state of health, terrible detention conditions, and the judiciary’s inaction with regard to the complaints filed.”[58] Moreover, even those jails and prisons that are purportedly willing to provide gender-affirming health care, but that require a gender dysphoria diagnosis or history of medical intervention, inappropriately exclude a number of transgender and non-binary prisoners who need gender-affirming treatment. Importantly, not all individuals who identify as transgender or gender nonconforming experience gender dysphoria; in other words, some people do not feel discomfort in their bodies, with or without medical intervention. Regardless of a diagnosis of gender dysphoria, however, many incarcerated individuals have medical needs specific to their gender identity and expression as well as their medical history. For example, prior to incarceration, many transgender and non-binary prisoners have undergone some type of gender-affirming medical treatment, such as hormone therapy, and need continued treatment for medical and mental health reasons. In one U.S. study, “more than a third of transgender, nonbinary gender, and Two-Spirit respondents took hormones prior to their incarceration,” but the majority of those individuals took street-based hormones that were not prescribed by a doctor, and thus have no record of this treatment. Of the respondents who had previously been taking hormones, 44% were denied access to those hormones in prison.[59] Prisons should not abruptly discontinue hormone therapy for transgender and non-binary people, regardless of whether that treatment was prescribed, as doing so could endanger their physical and mental health. Similarly, prisons should not deny transgender people gender-affirming medical care simply because they have not previously received a gender dysphoria diagnosis or transition-related treatment.[60] Restrictive policies that limit treatment to those with a specific diagnosis or prior medical record therefore prevent many individuals from accessing critical gender-affirming health care in prison. It is important that defense teams respectfully and sensitively discuss clients’ medical and mental health needs[61] as well as their desires for how to obtain the gender-affirming care required to meet these needs. Defense teams should be aware of the DSM-5 and ICD-10 descriptions of disorders and/or conditions related to gender identity and expression, the prevailing standards of medical care for transgender and gender diverse people, and the laws and policies pertaining to the provision of adequate medical care in the relevant jurisdiction.
Violence in Prisons and Police Stations
Women prisoners often suffer sexual harassment and violence. Although international standards require that women prisoners remain under the authority of female prison staff, prisons do not always respect these norms. Prison guards may subject women prisoners to rape, sexual touching, intrusive pat-downs and strip searches, and other forms of sexual humiliation. In some regions, guards may extort women into providing sex in exchange for special privileges. In Tanzania, for example, human rights advocates report that there are “transactional relationships” between some male guards and female prisoners where inmates receive protection and food in exchange for sex.[62] Women are also vulnerable to sexual violence in police stations. Women who are held on criminal charges may be raped, tortured, or subjected to sexual humiliation, such as being forced to strip before male officers.[63] Defense teams representing women need to ask them about their experiences in police stations and prisons to ascertain whether they have experienced sexual violence. Women may be reluctant or ashamed to report these experiences, and defense attorneys need to be patient and gentle in eliciting women’s accounts (see Chapter 4). Women may fear exposure and humiliation, and may need reassurance that you are bound by attorney-client privilege not to share any information they provide. Above all, it is essential that you overcome any discomfort in speaking to your client about her experiences of sexual assault or abuse. If you do not specifically ask whether your client has experienced sexual harassment, coercion, or violence, she may never tell you. “Why do male guards work where we eat, sleep, shower, and groom? It’s too much power. I’ve seen girls show their breasts for an extra cup of water.” —Kwaneta Harris, currently incarcerated.
LGBTQ+ Women Prisoners
All LGBTQ+ women prisoners—and trans women in particular—face heightened rates of discrimination, abuse, and sexual assault from the moment that they come into contact with the criminal justice system.[64] As an initial matter, there is a long history of police violence against LGBTQ+ women globally.[65] For example, a U.S. study in 2015 revealed that 58% of transgender people who interacted with law enforcement in the last year reported experiences of harassment, abuse, or other mistreatment by the police.[66] More recently, in Cameroon, security forces arrested at least 27 people from February to April 2021 for “alleged consensual same-sex conduct or gender nonconformity,” sometimes beating those arrested and subjecting them to forced anal examinations.[67] Similar violations have been reported in countries around the world.[68] Violence against LGBTQ+ people is perpetrated both by staff and other inmates. In the U.S., for example, more than one in three LGBTQ+ prisoners was physically assaulted by staff, one in ten were pressured to provide sexual favors, and one in ten was sexually assaulted by staff.[69] Abuse and violence committed by other inmates is even more prevalent, with one U.S. study reporting that 59% of transgender women housed in men’s prisons were sexually abused.[70] Such pervasive patterns of violence have been documented worldwide.[71] Transgender women also experience higher rates of strip searches and report that strip searches are frequently used as a tool of humiliation, abuse, and control.[72] In a 2014 report by Human Rights Watch, a Malaysian trans woman described how she was arrested under a cross-dressing law, subjected to an anal exam, told to strip naked, and “paraded from one cell to another so other inmates could look at her breasts.”[73] This woman’s experience is illustrative of a widespread practice of abuse. Importantly, while much more limited strip searches have generally been affirmed as necessary for security, the constant invasion of a transgender prisoner’s body in any form can be devastating. What’s more, when LGBTQ+-identifying female clients report abuse, they are often disbelieved, dismissed, or blamed for the abuse by staff. Trans women prisoners who have been assaulted report that staff often express that the prisoner deserved to be victimized or was “asking for it.” Additionally, upon reporting abuse, LGBTQ+ clients are often subjected to selective, arbitrary, and indefinite solitary confinement or other form of retaliatory punishment.[74] Defense teams must be aware of the heightened risk of discrimination, abuse, and violence by both other prisoners and staff when representing LGBTQ+-identifying female clients and, in turn, advocate for their clients’ safety and fair treatment. Defense teams should also be aware of the ways in which other countries have acknowledged the unique vulnerabilities of transgender and non-binary prisoners and the steps they have taken to address those vulnerabilities. For example, in Argentina and Chile, “courts have granted trans women alternative measures to the deprivation of liberty, such as house arrest, taking into account their life stories and trajectories, the exceptional nature of the situation of vulnerability that they experience in prison, health reasons, exposure to violence, and the lack of a gender and sexual diversity perspective in the judicial system.” Colombia has developed guidelines stipulating that “detained trans people must be consulted, on a case-by-case basis, as to whether they prefer to be searched by a man or a woman,” and has even crafted provisions specific to visitors to a prison that require personal searches “be conducted on the basis of the gender declared by that visitor, regardless of what their identity document says.”[75] Such policies acknowledge the importance of a person’s gender identity and bodily integrity.
Chapter 3: Women and Mental Health: Considerations for Defense Teams
“The system wants you to recount every traumatic incident you’ve survived. But what happens when you’ve spent your life running from that pain? What if you’ve been silent for so long, you’re not capable of speaking about it?” —Kwaneta Harris, currently incarcerated. Mental illness is endemic in the incarcerated population. Mental illnesses such as schizophrenia, post-traumatic stress disorder, and bipolar mood disorder affect an individual’s ability to form the intent to commit a crime and may render her incompetent to stand trial. If she is found guilty, your client’s mental disability often affects her moral blameworthiness, providing a powerful argument for a reduced sentence. [76] Nevertheless, few attorneys understand the relationship between gender and mental health. This is perhaps not surprising, since most mental health research has failed to account for gender-specific differences in the etiology and symptomology of mental illnesses. Yet women’s mental health affects their pathways to incarceration and their ability to tolerate certain conditions of confinement in ways that are distinct from men.[77] For example, incarcerated women have a greater incidence of serious mental illness than men, higher rates of substance dependence, and are more likely to have suffered past physical and sexual abuse.[78] As a result, practitioners must evaluate the mental health of their women clients through a gender-sensitive lens. This chapter will help you develop a gender-specific approach to assessing your client’s mental health. Rather than providing a comprehensive guide to mental health in capital cases, it focuses on the mental illnesses that commonly affect women charged with crimes. We highlight how each of these illnesses can affect a woman’s behavior, and provide advice to practitioners on navigating these mental health challenges with their women clients. This chapter is intended both as a guide and a resource to aid practitioners in providing gender-sensitive representation for women defendants. It is not intended to provide comprehensive diagnostic criteria, nor should it serve as a substitute for consulting with a competent mental health expert. Rather, our hope is that after reading this chapter, you will be better able to recognize the signs and symptoms of mental illness in your female clients and take steps to preserve their rights in the course of your representation.
Intellectual Disability and Gender
The case of Grace Banda (not the client’s real name) provides a good example of how lawyers presented evidence of intellectual disability to obtain a reduced sentence for their client. Grace, an intellectually disabled grandmother, was sentenced to death in Malawi in 2003. Grace’s mother regularly drank alcohol during her pregnancy, and as a result Grace suffered from Fetal Alcohol Spectrum Disorder (FASD). Additionally, she was malnourished as a child and her growth was stunted as a result. Grace attended three years of primary school but was unable to learn how to read or write. She eventually married, but left her husband after he started beating her and having relations with other women. During a famine in her village, her grandsons stole maize from a neighbor’s field. One of the boys, suffering from malnutrition, died from the beating she inflicted to discipline him. She attempted to revive him to no avail, and reported the incident to the authorities. After spending thirteen years on death row, Grace was granted a sentence rehearing in 2016. At that time, a neuropsychiatrist evaluated Grace and concluded that she was intellectually disabled. Based in part on her intellectual disability, the High Court reduced her sentence to a term of years. Already elderly and in poor health, Grace was released on humanitarian grounds in 2018.
Women and Trauma
“One of the most consistently reported risk factors for PTSD is being female.”[79] Women are more likely than men to experience trauma, including rape, intimate partner violence, and other forms of gender-based violence,[80] and this risk of trauma is heightened for women with multiple marginalized identities.[81] The World Health Organization estimates that one in three women worldwide have faced sexual or physical violence by either an intimate partner, non-intimate partner, or both.[82] For this reason alone, practitioners need to understand common sources of trauma and their impact on women’s mental health and daily functioning. Research shows that women more frequently “report an impact on their functioning” related to the trauma;[83] and are at a higher risk of developing certain conditions associated with trauma.[84] Criminalized women have experienced trauma at higher rates than women in the general population—and at higher rates than the male prison population. According to one study, more than 57% of women “in state prisons and 55% of women in local jails report having been physically and/or sexually abused in the past.”[85] But other studies indicate that experiences of gender-based violence among incarcerated women are far more widespread: one 1999 study concluded that over 80% of women at Bedford Hills Correctional Facility in New York had experienced physical or sexual abuse during their childhood, and over 90% had experienced abuse before their incarceration.[86] Responses to trauma vary. They include behavioral, physical, biological, emotional, cognitive, and other reactions. Repeated, severe trauma often results in a trauma-related mental disorder such as PTSD.[87] As an advocate, you must learn to recognize the symptoms of trauma in a client, as they can affect virtually every stage of your client’s contact with the criminal legal system. This section will begin by exploring common sources of trauma for women who are charged with serious crimes. It will then provide a brief overview of mental disorders that result from trauma, exploring common signs and indicators. Finally, the section will provide practical guidance for capital defense lawyers defending female survivors of trauma.
Sources and Symptoms
Sources of Trauma and Adverse Childhood Experiences
Women in prison have often experienced multiple traumatic events; one study found that incarcerated women experienced on average six different types of trauma in their lifetime.[88] Common sources of trauma for incarcerated women include experiences with interpersonal violence, including physical and sexual violence in childhood and adulthood.[89] These traumatic experiences can also lead to depression, PTSD, and substance dependence. The more trauma that a woman experiences, the more likely she will develop these conditions.[90]
| ACES | EXAMPLES |
| Neglect | § Emotional neglect § Physical neglect |
| Abuse | § Physical abuse § Sexual abuse § Emotional abuse |
| Household Challenges | § Mother treated violently § Household substance abuse § Household mental illness § Parental separation or divorce § Incarcerated household member |
Adverse Childhood Experiences (“ACEs”) are also prevalent among incarcerated women.[91] The graphic below provides an overview of ACEs that were developed by researchers in the United States. ACEs are traumatic events that occur before the age of 18. Researchers often group ACEs into three categories: neglect, abuse, and household challenges.[92] In addition to the common list of ACEs below, some studies include poverty, community violence, and death of a parent as additional experiences.[93] Incarcerated women are not only more likely to have experienced ACEs than women who have never been incarcerated, but also more likely to have suffered multiple events.[94] Moreover, girls involved in the criminal legal system are more likely than boys to have suffered an ACE, and are more likely than boys to have suffered multiple ACEs.[95] The more childhood trauma a woman endures, the more likely she is to engage in criminal behavior, suffer interpersonal violence in adulthood, and develop post-traumatic stress disorder and related symptoms.[96] While the ACE questionnaire may be a good way to assess potential childhood trauma in a client, it is only a starting point. The ACE questionnaire does not measure for “degree, duration, severity, timing, or quality” of each experience,[97] and as mentioned above, repeat exposure to traumatic events compounds its harm on the individual. Moreover, the ACE framework was developed to assess the lives of children in the United States, and there may be other adverse childhood events that have greater significance in your country.[98] For example, widespread drought, with accompanying malnutrition and death, is a significant childhood experience. Experiences of armed conflict also have unique and devastating consequences on girls and women alike. In order to understand the sources of trauma in your client’s life, you will need to spend time obtaining a thorough life history.[99]
Common Symptoms of Trauma
Most women facing the death penalty will have suffered repeated trauma over the course of their lives. After enduring trauma stemming from physical, sexual, and/or psychological abuse or neglect, women frequently experience post-traumatic stress.[100] “Simple” post-traumatic stress often occurs after a one-time incident, while “complex” post-traumatic stress develops from persistent, long-term abuse, typically from caregivers and during early life stages. Complex post-traumatic stress may also occur in adulthood as a response to frequent abuse by a partner over years.[101] Typically, people who experience severe abuse will have both simple and complex post-traumatic stress.[102] Further, trauma is cumulative: repeated exposure to traumatic events exacerbates their impact and leads to heightened symptoms.[103] While not everyone who experiences a traumatic event will develop post-traumatic stress disorder, women are twice as likely as men to develop it.[104] Furthermore, LGBTQ+ women experience higher rates of PTSD than heterosexual and cisgender women.[105] One study showed that over 50% of incarcerated women met the criteria for PTSD.[106] Women who have simple post-traumatic stress may have nightmares, flashbacks, feelings of numbness, disinterest in daily activities, constant vigilance, or avoidance of events that remind her of the traumatic experience.[107] Women who suffer from complex post-traumatic stress may have feelings of despair, worthlessness, depression, unexplained shame or guilt, problems trusting others, susceptibility to emotional outbursts and impulsive behaviors, feelings that life is meaningless, an inability to relax, persistent sleep problems, and feeling like they are not entitled to happiness.[108] In response to these emotions, women may abuse drugs or alcohol, cut or burn themselves in self-harm, or isolate themselves from others because they feel safer alone. They may also try to please others to avoid conflict, another person’s anger, disappointment or hurt.[109] It is worth mentioning that trauma can cause or exacerbate a variety of other mental disorders, some with unique behaviors or symptomologies. Symptoms of severe trauma vary, but the following are extremely common: emotional numbing, hypervigilance, dissociation, somatic symptoms, and intrusions.[110] The table below provides an overview of each symptom:
| SYMPTOM | DESCRIPTION |
| Emotional numbing | Emotional numbing refers to a reaction where a person detaches their emotions from “thoughts, behaviors, and memories.” A person experiencing numbing may display few emotional reactions and may speak with a “flat affect,” or in a “matter of fact” manner. |
| Dissociation | Dissociation is a symptom where people “lose focus” on the present. They may enter a sort of auto-mode, severing the connection between “thoughts, memories, feelings, action, and sense of identity.” Evidence of dissociation includes “fixed” or “glazed eyes,” sudden flat affect, prolonged silence, “excessive intellectualization,” and responses that seem inappropriate for the situation. |
| Hypervigilance | Hypervigilance, also known as hyperarousal, is a symptom where the body is in a state of preparation for danger. It often presents through physical symptoms like sleep issues, tension in the body, and a lower threshold for startle responses that remains for a long period after the traumatic experience. Hypervigilance is also a primary diagnostic criterion of PTSD. |
| Somatic symptoms | Somatic symptoms or bodily symptoms of trauma can include sleep, digestive, heart, brain, muscle, skeletal, breathing, skin, urological, and substance abuse issues. Emotional distress may present through these physical symptoms. They are particularly common in persons with PTSD. |
| Changes in brain development and cognitive functioning | Changes in brain development and cognitive functioning are symptoms that may materialize in various ways. One might perceive a safe situation that reminds them of a traumatic event as dangerous, experience excessive or inappropriate guilt, including survivor’s guilt, idealize or feel compassion for perpetrators through trauma bonding, experience hallucinations or delusions, or have intrusive thoughts. Trauma survivors may also “feel different” from others, feeling they can only relate to persons with similar traumatic experiences. |
| Intrusion | Intrusion may include triggers or flashbacks. Triggers are sensory reminders of trauma; they can include smells, noises, physical touch, views, or other sensory intakes that “cause strong emotional or other reactions.” Flashbacks are a re-experiencing of a trauma as though it was happening in the present. While they are typically short, the “emotional after-effects” can last for hours.[111] |
Dissociative Disorders are also common among people who suffer from complex or repeated trauma.[112] Women with “dissociative amnesia” may forget autobiographical details or memories. A woman who experiences “depersonalization” or “derealization” may have feelings of unreality, or repeated detachment from herself or her environment. These symptoms have important consequences for the attorney-client relationship. For example, when you discuss your client’s experiences of trauma, it may trigger dissociative responses.[113] Clients may also experience amnesia or shame, leading them to disavow a previous narrative she may have reported.[114] She might also “shut off” when discussions of her trauma become emotionally overwhelming.[115] The following section will include ways to help a client who experiences these and other symptoms.
Trauma and Representation
Trauma affects each part of a capital defendant’s experience in the criminal justice system, from arrest to incarceration. This section will focus on the effect of trauma symptoms in relation to representation, highlighting common difficulties you and your client might face, and offer practical guidance to help combat potential harms in and outside of the courtroom.
Inconsistent Testimony
Trauma affects a woman’s ability to offer a cohesive narrative. In the courtroom, judges and juries tend to look for internal and external narrative consistency. Internally consistent stories are emotionally and logically coherent, linear, and whole.[116] Externally consistent stories mold to the way a typical person might understand the world.[117] Because of psychological and neurological trauma, your client may struggle to recall experiences or act in ways that conform to the court’s expectations. Because trauma may affect your client’s memory and sense of self,[118] she may struggle to tell an internally consistent story. Dissociative states or lapses in memory make it difficult to recall events or tell a linear narrative.[119] Clients who suffer from certain dissociative disorders are prone to autobiographical amnesia;[120] they may not be able to remember certain events or periods of their life. When a client recalls traumatic memories, the memories “often lack verbal narrative detail and context.”[121] A client may experience the memory “in the form of sensations, flashes, and images, often with little or no story,” rendering it difficult to communicate the experiences to the court.[122] Unable to place her own memories on a timeline, she will find it exceedingly difficult to communicate what happened in a linear fashion to the court. Additionally, your client may experience intense emotions when recalling the trauma; as a result, she may forget, skip, or be “unable to speak key details” of the story.[123] Trauma may also affect your client’s decisions or behaviors, creating stories that seem to be externally inconsistent. As we explain in Chapter 4, women who experience various forms of abuse may not report the abuse to authorities and often remain with their abusers for various psychological, emotional, financial, and other reasons.[124] Judges and other courtroom actors tend to treat this behavior as evidence that negates a narrative of abuse.[125] Viewing the world from their perspective, judges implicitly or explicitly ask themselves “why would she stay?” or “why didn’t she ask for help?”[126] Additionally, judges, mostly male non-survivors, tend to discount psychological harm and concentrate on physical harm of victims.[127] If your client leads her testimony with experiences of psychological or emotional harm, courtroom actors may consciously or subconsciously discredit or discount the abuse, even if it is the most salient form of her trauma.[128] In a non-trauma-informed courtroom, testimonial inconsistency is especially harmful: courtroom actors, including judges, officers, and jurors, will question your client’s credibility and view her narrative as “suspect,” thereby harming your case.[129] You must anticipate that your client may suffer from memory gaps or inconsistency, and you must not assume that your client is dishonest or unintelligent. As discussed below, it will be necessary to educate the court on why trauma survivors are apt to give inconsistent statements about traumatic events and act in ways that do not conform to society’s expectations.
Client Demeanor
The symptoms of trauma, notably hyperarousal, numbness, and intrusion, may affect a client’s demeanor in the courtroom or before law enforcement.[130] Without trauma training, legal actors may misinterpret these reactions and judge her as cold and unemotional. This can further damage your client’s credibility. A survivor who responds to trauma through emotional numbing may recount her experiences in a flat, uninvolved, or matter-of-fact tone (also known as “flat affect”).[131] When she gives testimony, she may appear to those around her as callous or unremorseful when discussing details of her alleged crime.[132] A client experiencing hyperarousal, or the “anxious posture of alertness and reactivity to an imminent danger,” on the other hand, may appear “highly paranoid” or overemotional.[133] The client may further experience “unexpected outbursts of rage in response to relatively minor incidents,”[134] potentially miscommunicating to the jury or judge that they are violent or dangerous. Intrusion, or reliving of trauma, notably in the form of flashbacks, may prevent a witness from testifying about events in a chronological and consistent manner.[135] To the non-trauma-informed court, a client’s emotional or non-emotional reaction may affect the court’s assessment of her character or the credibility of her testimony: “Because PTSD symptoms can make abused women appear hysterical, angry, paranoid, or flat and numb, they contribute to credibility discounts that may be imposed by police, prosecutors, and judges.”[136] An untrained judge or prosecutor may weaponize the client’s demeanor, or the evidence of her trauma, in the courtroom, suggesting the client is guilty, unremorseful, and inhumane.
False Confessions
A survivor’s experience of physical and psychological trauma may increase the likelihood that she will falsely confess to criminal behavior.[137] One study of adolescent women explained that the strongest predictor of false confessions for females was psychological or physical trauma, including viewing physical violence in the home.[138] The study concluded that fear of negative or difficult interactions with authority figures from these experiences increases the risk of false confessions.[139] Survivors of domestic abuse in particular are “more vulnerable to authoritarian police investigation, [more likely to] get confused, and believe promises similar to battering relationships.”[140]
Violence, Trauma, and Suggestibility in Police Interrogations of Women
Melissa Lucio, a victim of childhood sexual abuse and domestic violence, was wrongly convicted and sentenced to death in Texas for the death of her toddler daughter. Her mother’s boyfriend began abusing Melissa when she was only six years old. For two years, he abused her regularly, and when she told her mother, her mother didn’t believe her. As a teenager, Melissa was raped by a stranger. Traumatized and desperate to escape her home, Melissa married at age sixteen. Her husband was a violent man who also abused Melissa and eventually abandoned her after she bore five children. Melissa’s next partner continued the cycle of violence. During this time Melissa had seven additional children. Like many victims of sexual abuse and domestic violence, Melissa developed Post-Traumatic Stress Disorder and Depression. She began to dissociate under stress, and became passive and avoidant when confronted, especially when those confronting her were stronger than her. While Melissa and her large family were moving, Melissa’s daughter fell down a full set of outdoor stairs, landing on the cement at the bottom. Several of Melissa’s other children witnessed this fall. Days later, Melissa’s daughter became lethargic, went to sleep and never woke up. Melissa was immediately arrested and interrogated. She denied harming her daughter. The police insisted she was guilty, aggressively interrogating her until 3 a.m. Finally, Melissa told them what they wanted to hear–that she was responsible for her daughter’s injuries. At trial, the court refused to let Melissa’s defense lawyer present expert testimony explaining why a victim of repeated sexual abuse and domestic violence would be more likely to falsely confess. The Innocence Project submitted a brief in the U.S. Supreme Court in support of Melissa, noting that “[w]omen with abuse histories, like Ms. Lucio, [are] particularly vulnerable to false confessions.” The Innocence Project further noted that “false confessions are prevalent in cases involving child victims,” particularly when the defendant has a history of trauma. But the jury who sentenced Melissa to death did not know this, and Melissa remains on death row and at risk of execution. A study on gender differences in false confessions suggests that women who make false confessions “are more likely than men to have trauma backgrounds,” “are more likely involved in crimes against children,” and often make such confessions to “protect the abuser out of love [or] fear,” and “internalize guilt about not protecting children due to their own abuse and inability to persuade [the] batterer to seek help.”[141] These findings reiterate that past and present trauma may affect a survivor’s vulnerability to police pressure to confess.
Considerations to Mitigate Harm
If you are able to educate prosecutors, judges, and jurors to the causes and symptoms of trauma, and your client’s psychological and neurological symptoms—including numb or emotional demeanor— false confessions, and inconsistent testimony may be taken as evidence of trauma instead of deceitful or guilty conduct.[142]
Presenting Expert Testimony
Expert testimony is often necessary to provide jurors or judges with the right framework to understand trauma and its presence in the courtroom.[143] An expert may testify about symptoms of trauma, explaining the symptoms in plain language and in a relatable way.[144] Expert witnesses in cases of interpersonal violence are particularly important. Beyond providing direct testimony, they can assist in assessing the police interrogation and its impact on your client, they can help prepare your client for trial, and assist with jury selection.[145] Testifying witnesses can also dispel common myths about trauma survivors—including, for example, the reasons women may remain in violent relationships.[146] Experts can help explain common questions that juries and judges have, including why a trauma survivor would be more susceptible to coercion by a male co-defendant, or why she may have acquiesced in the abuse of her children.[147] Ultimately, experts may also provide context for your client’s non-linear, inconsistent testimony, her lack of emotion (or hyper-emotional responses) in the courtroom, and other emotional, mental, and behavioral symptoms that a client demonstrates which might undermine her credibility to the observer unfamiliar with the effects of trauma.
Asking the Right Questions and Building Trust
“I am not expecting my lawyer to be a therapist, but having basic understanding of trauma goes a long way. I would not have resisted my attorney’s questioning about my experiences if I understood what they were going to do with the information.” —Kelly Savage, formerly incarcerated woman and survivor of domestic violence. “If a client tells you they are innocent, believe them.” —Debra Milke, formerly incarcerated woman on death row, wrongfully convicted of murdering her son. As mentioned above, it is often difficult for survivors of trauma to tell a cohesive, linear narrative. In order to uncover your client’s trauma history, you must first build a relationship of trust. Your client may not feel safe speaking to you. She may not trust you, or she may not feel able to express herself or share details of her history. You will need to be patient, and take the time to build a relationship where your client feels safe with you. You should be transparent, predictable, and reliable. You must support your client while allowing her to exercise control of her situation.[148] In order to help your client feel safe, it is important to communicate each step of the criminal process to your client. Communication with judges or other figures of authority, conditions of detention, or the testimony of others may trigger trauma responses for your client. It is important to tell your client what she should expect at each stage of the process to help her prepare for these moments. Simply using your client’s own terminology instead of professional language can help your client feel more comfortable and heard.[149] When a client experiences a trigger, it is important to help your client distinguish the past and present; grounding techniques are particularly helpful. We have included a few techniques below for your use. Normalizing the events, as well as offering information about flashback and triggers, can help you and your client discuss potential causes, and therefore avoid re-traumatization in the future. Small acts, like giving your client time and space to speak or offering her food or a beverage can help create a comfortable atmosphere. You can always ask your client directly if there are particular activities that make her feel calm or safe, and invite her to do them.
| Technique | Examples |
| Grounding activities | 5, 4, 3, 2, 1: Ask you client to name five things she can hear, then five things she can see, then five things she can feel in the room. Repeat the exercise by asking her to find four new things, then three, two and one thing.[150]
Categories: Have your client choose a category (e.g., colors, objects), then ask her to point out objects from that category in the room.[151] |
| Guided meditation | Progressive muscle relaxation: Ask your client to close her eyes and breathe slowly. Then, ask her to focus on various body parts. As she focuses on one, ask her to breathe out the tension she might feel there. |
| Breathing exercise | 3-3-3: Ask your client to breathe in for three seconds, hold for three, and exhale for three. Repeat as desired. |
Postpartum Mental Disorders
Whenever you are defending a woman charged with killing her child you should explore whether she suffered from postpartum depression or psychosis. Although these conditions are not uncommon, they are widely misunderstood. The case of Debra Gindorf in the United States is illustrative. Debra was sentenced to life without the possibility of parole in 1986 for killing her two children. Of the nine mental health experts who evaluated her, all agreed that she suffered from some form postpartum psychosis.[152] Yet at the time of her trial, the judge largely ignored Gindorf’s experts, and relied on witness testimony that Debra, although slightly depressed in the months after childbirth, did not seem “psychotic.” In 2009, in a victory for postpartum advocates, the Governor of Illinois finally commuted Gindorf’s sentence and ordered her released for time served. Postpartum mental disorders remain an under-explored form of mental illness in mothers. There is no one set of symptoms, nor is there a single set of experiences. What an individual mother goes through can vary from a few weeks of mild sadness to, in very extreme cases, a full psychotic break. This section provides a basic overview of postpartum mental disorders, symptoms, and risk factors, and their implications for the defense of women facing murder charges.
Postpartum Mental Disorders
For the practitioner, it is important to recognize that postpartum disorders exist along a spectrum. Also, the duration of symptoms varies by individual and mothers can experience severe mental distress up to a year after childbirth. Postpartum disorders can also be episodic; practitioners should be wary of judging their client’s behavior at the time of the crime by her current state of mind.[153]
Postpartum Depression
Postpartum depression is a major depressive disorder that can appear anywhere from two weeks to a full year after childbirth. The fifth edition of the Diagnostic and Statistical Manual has a heading for postpartum disorders under the general heading for ‘Major Depressive Disorders.”[154] Practitioners should know that this conflation is at odds with clinical and medical literature, which treats postpartum disorders as a distinct category of mental illness.[155] If left untreated, postpartum depression can last for months. Some researchers have estimated that it affects anywhere from 13-19% of childbearing women.[156] Significantly, women who suffer from postpartum depression may develop intrusive thoughts of harming themselves or their baby and recurrent thoughts of suicide.[157] There are two important risk factors that correlate with postpartum depression: prenatal depression and ongoing physical, verbal, or emotional abuse.[158] Additional indicators for postpartum depression include stressful life events, marital conflict, young maternal age, low income, and being an immigrant.[159]
Postpartum Psychosis
The most severe postpartum disorder is postpartum psychosis. This extreme condition can develop within the first few weeks after delivery, but each case will be different, and symptoms may continue episodically for months after childbirth.[160] Postpartum psychosis is very rare and may affect around 1 in 500 mothers.[161] Symptoms, however, are extreme, and include:
- Confusion and disorientation
- Obsessive thoughts about the baby
- Hallucinations and delusions
- Sleep disturbance
- Excessive energy and agitation
- Attempts to harm themselves or their baby[162]
Risk factors for postpartum psychosis include a previous history of postpartum psychosis, previous psychotic episodes, a family history of psychosis, or bipolar disorder.[163] Postpartum psychosis is treatable, but it is a severe mental illness necessitating possible hospitalization and psychotropic medicine.
Postpartum Disorders in Criminal Trials
Postpartum disorders are relevant in capital defense at both the guilt and penalty phase. If the case involves infanticide, practitioners should conduct a thorough investigation for any possible postpartum psychosis or depression. Because postpartum disorders can go undiagnosed, and because so many people are unfamiliar with the disorders, retaining a qualified expert is essential. Capital defense lawyers will typically raise postpartum disorders—and particularly postpartum psychosis—by way of an insanity defense.[164] In the United States, several women have been found not guilty by reason of insanity based on their postpartum disorders.[165] If your client is convicted of murder notwithstanding her postpartum disorder, you should argue that her illness justifies a lenient sentence.
Gender Differences for Serious Mental Illness
There is still much work to be done in the study of gender differences surrounding mental health. While recent studies have begun to look at gender differences, the research is far from complete. What we do know is that, as noted above, incarcerated women have a higher prevalence of mental illness than men. Moreover, LGBTQ+ women and women with multiple marginalized identities experience higher rates of depression, anxiety, PTSD, and substance abuse.[166] What many lawyers do not know is that there are also striking gender differences when it comes to the development and symptoms of mental illness.[167] Gender differences exist in the age of onset of symptoms, frequency of psychotic symptoms, content of delusions, life course of disorders, social adjustments, and long-term treatment outcomes. There are many reasons that your client may not have received a prior diagnosis of mental illness, including institutional and financial barriers to accessing health care, lack of cultural competency, and discrimination and bias in the medical community.[168] For this reason, it is important to ask your clients open-ended questions about their actual lived experiences, both in terms of symptoms they have experienced and when those symptoms began. In essence, you must become an expert on your client’s mental health, as mental health evaluations provided at state-run hospitals tend to be narrowly focused on answering legal questions relating to concepts such as “sanity” and “fitness to stand trial.” These kind of evaluations will not provide a comprehensive, holistic assessment of your client’s mental health. Indeed, doctors successfully identify less than half of people who meet diagnostic criteria for psychological disorders.[169]
Case Study: Sex Differences in Schizophrenia
The U.S. National Institute on Mental Health defines schizophrenia as a mental disorder characterized by disruptions in thought process, perceptions, emotional responsiveness, and social interactions. Schizophrenia is typically persistent and can be both severe and disabling.[170] The symptoms of schizophrenia emerge earlier in men than they do in women. This is consistent across cultures, diagnostic criteria, and definition of onset. While the onset of symptoms in men peaks between ages 15-25, women have two ages of onset, peaking both between 15-30 and again at 45-49. Mean age of onset in broadly defined schizophrenia (under the International Classification of Diseases and Related Health Problems-9) is 31.2 years for men and 41.1 years for women. Symptoms between schizophrenic men and women differ substantially. Schizophrenic men are more likely to experience negative symptoms, such as social withdrawal, lack of motivation, and blunted speech. Women, by contrast, are more likely to experience atypical psychotic or affective symptoms such as dysphoria, depression, inappropriate affect, hostility, irritability, sexually inappropriate or bizarre behavior, and sexual delusions.[171] Women are also more likely to experience persecutory delusions than men and are more vulnerable to cycloid psychosis (a term used to describe psychosis that does not meet the criteria of either schizophrenia or bipolar affective disorder).[172] Women are also much more likely to experience auditory hallucinations than men.[173]
Gender Differences in Disease Onset and Symptoms
There is very little current research on gender differences in symptomology and age of onset between the sexes. Much like the case study above on schizophrenia, studies have shown sex differences in bipolar disorder. In one study, UK researchers monitored men and women’s experiences with bipolar disorder over the course of 35 years. They found that symptoms of bipolar disorder emerged sooner in men than women, even when adjusting for premorbid variables (variables that existed prior to the first onset of psychosis), including factors such as education, socio-economic status, and access to health care. The authors concluded that men had a higher incidence of bipolar disorder in early adult life, and women had a higher incidence throughout the rest of adult life until late life (although these differences did not reach statistical significance to allow for specific age brackets of expected occurrences).[174] Other studies have reached the same conclusion.[175] Symptoms of mental illness can be both physical and psychological. Sometimes, somatic symptoms of mental health conditions such as headache and palpitations may be disguising an anxiety disorder, or in other cases fatigue and muscle pain may have an underlying diagnosis of depression.[176] When women report symptoms, health providers often do not take their complaints seriously, in part because women are stereotyped as more emotional and more hypochondriacal.[177] This can lead to misdiagnosis or underdiagnosis of mental illnesses in women. For all those reasons, it is important to go through your client’s medical records carefully to identify any of these seemingly ‘physical’ conditions to determine if there is an underlying mental health condition that has been misdiagnosed.[178] It is equally important to talk to your client about any persistent symptoms they have experienced or reported which they may have been treated for, or were told it is “in their head” and there is nothing wrong.
Chapter 4: Gender-Based Violence: Myths and Misperceptions
“When I look at the women around me, I think about how every single one of them is here because of a man.” —Christa Pike, incarcerated on death row. Gender-based violence is ubiquitous in all cultures. It affects women of all social and economic backgrounds, in all parts of the world. Your client has likely experienced multiple forms of gender-based violence, so you must be prepared to engage with her about it and consider how her experiences have affected her life story and the offense itself. Gender-based violence is “violence which is directed against a woman because she is a woman or that affects women disproportionately.”[179] Gender-based violence also includes violence directed against transgender and gender non-conforming persons on the basis of their gender identity and expression. It encompasses a broad array of experiences, from vaginal rape and spousal violence to online harassment and controlling behaviors. Your client may have experienced more than one form of gender-based violence. Gender-based violence is endemic. One in three women around the world experience gender-based violence in their lifetime.[180] A 2018 analysis by the WHO estimated that 27% of women worldwide have experienced violence at the hands of a domestic partner.[181] Around 20% of women in both the United States and Europe have experienced rape or attempted rape.[182] Other forms of discrimination, such as those on the basis of race, ethnicity, sexual orientation, class, and gender identity, magnify the harms of gender-based violence.[183] Women who experience these intersecting forms of discrimination are more vulnerable to gender-based violence and less likely to receive support. The prevalence of gender-based violence is even more staggering in the criminal context: the great majority of women charged with serious offenses experience some form of gender-based violence before encountering the criminal justice system.[184] Many women serving serious sentences are repeatedly victimized. One study of people in the United States serving life without parole for youth offenses found that 80% of women respondents experienced physical abuse, 77% experienced sexual abuse, and 84% witnessed violence in the home before their incarceration.[185] A large proportion of women who are imprisoned for homicide offenses worldwide endure domestic violence, and many are imprisoned for killing their abuser.[186] The data alone thus suggests that your client’s background will include multiple experiences of gender-based violence. This chapter will help you begin to recognize and understand common forms of gender-based violence, including sexual abuse and domestic violence. First, the chapter will discuss why learning about your client’s experiences of gender-based violence is important to her representation and will cover the core terminology you will need to discuss these experiences. Second, the chapter will break down some common myths and misperceptions about gender-based violence, exploring sexual violence and then turning to domestic violence. In so doing, this chapter will help you understand the different experiences you should be alert to when speaking with your client and will develop your familiarity with issues that may arise in the context of her defense. Finally, the chapter will provide you with practical guidance on speaking with or interviewing your client about these sensitive topics. Although conversations about gender-based violence are often the most difficult, you have an important role to play in breaking the stigma around these topics, combating gender bias in the legal system, and giving your client a chance to tell her whole story.
Understanding Gender-Based Violence
Given the prevalence of gender-based violence in our clients’ lives, all criminal defenders must be equipped to understand the impact of varying forms of violence. Your client may not wish to share past traumas, she may not see her experiences as gender-based violence, and she may experience mental health complications as a result of abuse. Nevertheless, it is vital that you talk to her about her background. Gendered abuse affects women in many ways. Significantly, abuse can have a prolonged and detrimental impact on women’s mental health (see Chapter 3). These mental health complications can impair women’s judgment and reasoning. Abuse can also lead women to violence. The vast majority of women who use violence do so to defend themselves or their children, or to prevent an attack upon themselves or their children.[187] But even if women act violently against someone who is not their abuser, their acts are often attributable to the violence and trauma they have experienced.[188] In this way, violence against women is often a pipeline to prison.
Tanzanian Court Condemns Victim for Fighting Back Against Her Abuser
Chantal (not her real name) is a 35-year-old farmer, mother of four children, and survivor of brutal and repeated domestic violence. She was sentenced to death by hanging for protecting herself and her children from her abusive husband. His abuse was so violent that both Chantal and her daughter, on separate occasions, were hospitalized. One night Chantal’s husband came home drunk and started verbally abusing Chantal. He called her a “prostitute,” accused her of sleeping with other men, and threatened to kill her. She tried to calm him, but after the children went to sleep, her husband locked her in the bedroom. He repeatedly beat her with a stick and a hammer. During the beating, she managed to push him away. When he fell, she hit him with the hammer, causing his death. Chantal and her daughter testified about her husband’s abuse and his threat to kill her that night, but the court found her guilty of murder. The court rejected her explanation that she acted in self-defense and sentenced her to death. Because Tanzania has a mandatory death penalty, the court was unable to take into account Chantal’s history of victimization at the hands of her husband before sentencing her to die. She remains on death row because she dared to protect herself and her children from the abuse of her husband. The system failed to protect her from continued abuse, and despite plentiful evidence of her victimization and trauma, her children have been ripped away from her and left parentless. A mandatory death penalty for gender-based crimes of violence leaves only broken families and perpetuates the cycle of trauma. You must understand this link to provide your client with effective representation. Her experiences with violence will often provide information necessary for her full defense and mitigation of her sentence. Without a thorough understanding of these forms of violence, you risk overlooking important components of your client’s defense. Moreover, you must educate legal actors—including judges, prosecutors, and jurors—on the effects of gender-based violence, its connection to crime, and how your client’s background contributed to her actions. Prosecutors can use your client’s experiences of gender-based violence against her. For example, the state may use your client’s decision to stay with an abusive husband to discredit a claim of domestic violence, or prosecutors may characterize your client as a liar because she did not report a case of sexual abuse in her youth. Common law systems reward prosecutors for convictions,[189] thus setting up an incentive system for prosecutors to dismiss, belittle, and manipulate clients’ experiences of violence. You can respond to these arguments only if you have a good grasp of the issues yourself. All lawyers can fall prey to common misperceptions about gender-based violence, whether they are prosecution or defense-oriented, new or experienced, male, female, or another gender. Most defense attorneys have been raised in a society that normalizes and tolerates gender-based violence. This chapter will help you recognize your own internal biases so that you can provide effective, gender-sensitive legal representation.
| Dos: | Don’ts: |
| § Read up on gender-based violence and understand the terminology. § Be aware of how the judge, jury, attorneys, and investigators involved in the case may perceive your client and may attempt to portray her. § Be aware of your own biases, whether conscious or unconscious—adopt a methodical approach to overcome them and work with gender-sensitive experts where possible. | § Fall prey to common misconceptions about gender-based violence. |
Core Terminology
Before reading the remainder of this chapter, it will be useful to understand some of the core terminology used throughout. Gender-based violence (GBV): Harm that is inflicted because of a person’s gender or gender expression. GBV also refers to harm that disproportionately affects persons of a particular gender. The term usually refers to harm that disproportionately affects cis women and transgender and gender diverse persons. Violence against women (VAW): Violence which is directed against a woman because she is a woman or that affects women disproportionately. Victim/survivor: Women who are subjected to gender-based violence are often referred to as “victims” or “survivors.” Neither term is perfect. Victimhood risks characterizing a woman who has experienced abuse as helpless, passive, and pitiful; survivorship strives to empower women and recognize strength, but also oversimplifies the range of reactions a woman may have to abuse. Moreover, not all women “survive” abuse. This chapter will typically refer to women who have experienced abuse as “victims” because this framing may be strategically helpful for litigation, and because legal systems may expect women to present as paradigmatic victims in order to recognize their experiences of abuse (see “Sexual Violence: Myths and Misperceptions,” below). Note that some women prefer one term over the other. If your client has a preference for how you refer to her experiences, you should respect her wishes. Sexual violence: When a person forces or manipulates another into unwanted sexual activity. Examples of sexual violence include rape, sexual harassment, and unwanted sexual touching. The force involved does not have to be physical. Someone may force another into sexual activity because of fear or the victim’s age, illness, or incapacity. Rape: Rape is “a physical invasion of a sexual nature” that is committed on another person in coercive circumstances.[190] It encompasses the penetration, however slight, of any orifice of another person. Penetration can be with a part of the perpetrator’s body or with an object. Under international law, coercion includes any circumstances that render an act of sexual penetration non-consensual, and thus extends beyond the use of physical force.[191] Rape can be committed by a person of any gender against a person of any gender. Domestic violence: Also referred to as intimate partner violence. Domestic violence or domestic abuse refers to gender-based violence directed at a person by their partner or former partner, such as a spouse, boyfriend, or ex-boyfriend. Domestic violence can be perpetrated by a person of any gender. The term encompasses many different forms of violence. See “Domestic Violence: Myths and Misperceptions,” below. Psychological abuse: Also called emotional abuse. Psychological abuse refers to a person’s regular and deliberate use of a range of words and non-physical actions to manipulate, hurt, weaken, or frighten their victim.[192] These words can distort, confuse, and influence a victim’s responses in her everyday life, changing her sense of self and harming her wellbeing. Psychological abuse can be even more damaging to a victim’s mental health than physical violence. See “Domestic Violence: Myths and Misperceptions,” below. Coercive control: This term describes the constellation of behaviors used to restrain women’s liberty and monitor their behavior—to establish control over her behavior. It is typically used in the context of domestic violence. See “Domestic Violence: Myths and Misperceptions,” below. Economic abuse: Usually occurs in the context of a domestic relationship. Economic abuse refers to one partner’s control over the other’s finances. The abuser may restrict his or her partner’s access to money, controlling how she can spend money, and sabotaging her access to resources that would give her financial independence. Battered Women’s Syndrome: Battered Women’s Syndrome refers to a psychological cycle resulting from domestic abuse. The term was coined by psychologist Dr. Lenore Walker in the 1970s. Dr. Walker theorized that abused women go through a cycle of three phases: the tension building phase, in which tension builds between a perpetrator and victim through low-level conflict; a battering phase, in which the tension grows to physical conflict; and a honeymoon phase, in which the perpetrator tries to win back the victim’s affections. In the United States, Dr. Walker’s theory was incorporated into the legal understanding of domestic violence and continues to dominate courts’ understanding of domestic abuse. Anti-violence advocates have since called the theory into question, though, for its characterization of domestic violence as an easily-identifiable cycle of physical violence, for its failure to capture the complexities of different forms of violence that can and do occur in a domestic partnership, and for its characterization of a domestic violence victim as a passive non-actor with no agency.[193] Battered Women’s Syndrome characterizes women as fragile and passive, without accounting for survival actions they may take to protect themselves or their children. The cycle theory of violence is no longer widely embraced by domestic violence professionals, but it continues to influence the legal system.[194]
Sexual Violence: Myths and Misperceptions
This section will discuss some common misperceptions related to sexual violence. Sexual violence encompasses acts such as rape, attempted rape, unwanted sexual touching, and incest. Sexual violence can be committed by someone of any gender, against a person of any gender. Sexual violence against women is a global health problem of epidemic proportions. Race, class, sexual orientation, gender identity and expression, and other factors influence the likelihood that a woman will be subject to sexual violence in her lifetime. Low-income women are more likely to suffer abuse than more affluent women.[195] Global economic conditions also contribute to violence against women. In times of economic hardship, rates of violence against women increase.[196] Women belonging to racial and ethnic minorities are also victimized at higher rates. In the United States, for example, the prevalence of gender-based violence is highest among women of color. Approximately 44% of Black women and 46% of Native American women will endure sexual abuse in their lifetimes, compared to 35% of White women.[197] Women who are married as children[198] similarly face higher rates of victimization. Though tolerated—and even legalized—in many countries, child marriage is an act of gender-based violence under international law.[199] The African Court on Human and Peoples’ Rights has found that child marriage of girls constitutes impermissible gender-based discrimination and is a harmful practice under the Maputo Protocol and the African Charter on the Rights and Welfare of the Child.[200] Early marriage exposes girls to sexual violence by thrusting them into relationships with adults, who often expect sexual acts from their young brides for which they are neither physically nor emotionally prepared.[201] Child marriage thus increases the risk that the girls involved will have traumatic sexual experiences and will develop serious mental illnesses as a result of sexual violence (see Chapter 3).[202] Girls who enter into early and forced marriages are more susceptible to lifelong health complications because of their extreme vulnerability to sexual violence.[203] If your client was married as a child, you should argue that her status as a child bride is a factor to consider at the penalty phase. You must also consider that she has a high risk of exposure to sexual violence and other forms of gender-based violence. LGBTQ+-identified women face some of the highest rates of violence worldwide.[204] In 2020 alone, over 350 transgender people were murdered globally; of those killed, 98% were trans women or transfeminine people.[205] In the U.S., people of color made up 79% of all transgender people murdered; in Europe, 50% of those murdered were migrants.[206] Mentally disabled women are also subjected to higher levels of sexual violence.[207] You should educate yourself on different forms of sexual abuse. With sexual violence affecting millions of women the world over, especially women accused of serious offenses, it is important to develop fluency with issues relating to sexual abuse. Resources such as the World Health Organization’s webpage on violence against women or the webpage of the Rape, Abuse and Incest National Network (RAINN) on sexual abuse are useful tools for understanding common acts: https://www.who.int/health-topics/violence-against-women; https://www.rainn.org/types-sexual-violence. Many people have a general understanding of rape as forced sexual intercourse with a stranger, but the definition of rape is much broader. As explained below, it includes non-consensual sex with intimate partners and husbands. The definition of “rape” under international law (and under many national laws) also refers to more than vaginal penetration, and includes penetration of any orifice, however slight.[208] Thus, a man who forces his penis into a woman’s mouth is raping her; it would be incorrect to say that she is “performing oral sex.” Other forms of sexual violence are rarely discussed. For example, individuals who exercise direct control over a woman’s reproductive choices are engaged in a form of gender-based violence. Sometimes termed “reproductive abuse,” controlling a woman’s pregnancy is linked to abusive domestic relationships (see part 4 below), and often indicates that the victim experiences other forms of sexual violence.[209] Men can establish control over their partners’ lives by interfering with contraceptive methods (such as removing a condom or confiscating her contraceptive pills), or forcing a partner to terminate or keep a pregnancy against her wishes.[210] If your client indicates that her reproductive decisions were not her own, then you should be alert for other signs of sexual or domestic abuse. Other examples of sexual violence include “corrective rape,”[211] forced marriages,[212] and state-sanctioned sterilization of LGBTQ+ people.[213]
Examples of Gender-Based Violence
- Public humiliation
- Public yelling
- Demanding sex
- Threatening to hit
- Threatening to withdraw financial support
- Destroying personal property
- Refusing to provide payments
- Pushing, shoving, slapping
- Blows with a fist to the head or other parts of the body
- All beatings; beatings may leave bruising, swelling, fractures, or wounds
- Name-calling, persistent insults
- Controlling partner’s work, social, or family activities
- Blows during pregnancy
- Threats with weapons (guns, knives, etc.)
“Sex is a private matter”
Many of us grow up with the understanding that sex is a private affair and that all things relating to sex are private. In many cultures, speaking about sex is even considered shameful. This is particularly true of women, who often normalize the notion that their bodies and their sexual desires must remain hidden. For LGBTQ+ women, this stigma can be even more difficult to overcome, especially in instances where same-sex relationships and gender non-conforming identities are criminalized and subject to state-sanctioned or culturally-sanctioned punishment.[214] And in some communities, there is a lack of language[215] to describe same-sex relationships and identities as well as a lack of social recognition of those identities,[216] making it even more difficult for your client to communicate about their experiences and identities. As such, both you and your client may experience awkwardness, embarrassment, fear, and even shame when speaking about sexual activity. These feelings, especially humiliation or discomfort, are only amplified when speaking about sexual violence. Many women internalize feelings of deep shame after a sexual assault. Your client may blame herself, feel unclean, or even refuse to see what happened as sexual violence. Many studies on rape have shown that women try to minimize what has happened to them.[217] It is, therefore, all the more important that you approach conversations about sexual violence, sex, and intimacy with great care. You must not add to your client’s feelings of shame and you must not become awkward or avoidant yourself. The interview tips in section 5 provide some suggestions for approaching conversations about sex and sexual violence with your client.
“She was asking for it”
The idea of the “perfect victim” is a myth. Some popular misperceptions about victims of sexual violence include the notion that certain clothing or behaviors give consent for sexual activity. A commonly heard refrain around cases of sexual violence is that a woman was “asking for it” because she wore provocative clothing or flirted with her abuser. Critically, victims of sexual abuse do not invite abuse. A woman’s choice of clothing and behavior has no bearing on any sexual violence she experiences. Refrain from passing judgment about your client’s behavior and circumstances around her abuse. For many LGBTQ+ people who are victims of gender-based violence, their very identity is used as a legitimate reason for victimization. In many communities, sexual violence against LGBTQ+ people is considered to be an appropriate corrective measure or a lawful punishment for transgressing heteronormative norms.[218] In other instances, LGBTQ+ people are told that sexual violence is their fault, that they deserve it, or even that they must enjoy it since they are LGBTQ+.[219] Prosecutors have also embraced the stereotype of the “perfect victim;” in other words, a woman who is meek, submissive, and non-violent.[220] The perfect victim is unable to take any action to save herself, and survival action (such as killing her abuser) is criminalized.[221] This stereotype is important for defense teams to understand because often our clients are criminalized precisely because they took action to survive. There are class, race, and sexuality implications that underpin the stereotypical victim. Women who belong to minority communities such as sex workers, LGBTQ+ women, or women who are from certain racial groups, are often deprived of victimhood in the popular eye. In much of Europe and the United States, for example, the stereotypical victim is a “passive, middle-class, white woman cowering in the corner as her husband prepare[s] to beat her again.”[222] Black women are deemed too strong or hypersexual to be victims; women in same-sex relationships are forgotten in conversations about sexual violence; poor women are not deemed worthy of protection. The notion of the “perfect victim” is pervasive. Over the past 30 years, the public, the media, and the legal system have coalesced around this passive and non-violent stereotype of women subjected to abuse.[223] This “perfect victim” is not representative of the vast majority of women subjected to abuse. Because that stereotypical victim is what judges, juries, and prosecutors expect to see, though, women who defy the stereotype are at a distinct disadvantage. A woman who kills does not correspond with the victim story they want to hear. As your client’s advocate, you must overcome the stereotype of victimhood and find a compelling way to present your client’s story of abuse.
“She didn’t report it so it can’t be that bad”
There are many reasons why a woman may choose not to engage with law enforcement. As noted above, she may not view her experience as sexual violence, may be ashamed, or may be unsure about what happened. Many people also do not want the state to intervene in their sexual lives or relationships, especially when the abuser is someone known to the victim—as is all too often the case.[224] A woman is less likely to report an incident of sexual violence when she knows the perpetrator, sometimes through fear of the perpetrator, sometimes because she is socially or economically dependent on him, and sometimes because she loves him.[225] Some women do not have access to the resources they would need to support them in reporting abuse. Women who are socially or geographically isolated may not see reporting as a viable choice because they cannot communicate easily with law enforcement or because they have no access to a support network, such as friends or professional services. In rural communities, the people a woman would go to in order to report abuse may be people who know her or her abuser well. The abuser may be a respected leader in her community, or even a law enforcement officer. It can be difficult for women to bring such traumatic and personal experiences to authority figures whom she knows are close with her abuser. Mistrust of the police can also be a powerful factor for a woman who chooses not to report. Police forces have a history of oppressing certain minority groups in many countries around the world, which discourages people belonging to those groups from turning to the police for support in the wake of sexual violence.[226] Moreover, police often minimize, disbelieve, blame, or shame women who report sexual violence.[227] Police around the world have also committed acts of gender-based violence, including sexual violence. This is especially true for marginalized women—such as LGBTQ+ women,[228] poor women, and women of minority racial and ethnic backgrounds. Consequently, women from marginalized identities may be especially mistrustful of the police. Where trust in the police is low and people fear asking the police for help, victims are less likely to see reporting sexual violence to law enforcement as a viable option. Moreover, victims may not want to see the perpetrator imprisoned, but that is often the only solution the criminal justice system can offer. There are many reasons that a woman might choose to not speak of her experiences of sexual violence, much less report them. You must not judge your client’s decisions on this matter, nor can you draw any conclusions from them. Indeed, you should be prepared that your client may never have told anyone at all.
“It’s not rape if he’s her husband”
Many cultures across the world have historically refused to recognize rape or sexual assault by a woman’s husband. The notion that a woman is the property of her husband has long propelled the belief that a man cannot rape his wife. This is wrong. Sexual assault and rape can be committed by anyone, regardless of his relationship to the victim. Spousal rape is still rape, and you should still consider it an act of sexual violence. Section 4, below, covers acts of violence by a spouse in greater detail.
| Dos: | Don’ts: |
| § Normalize talking about sex; approach topics relating to sexual violence sensitively. § Use language that your client is comfortable with to describe her experiences but remember that she may also normalize acts of sexual violence. Be sure to obtain enough information so that you can assess whether she was subjected to rape or other forms of sexual violence. § Look for resources for your client; she may still experience the effects of sexual violence. | § Expect your client to conform to stereotypical notions of the “perfect victim.” § Dismiss your client’s experiences. § Imply that your client was in any way to blame for her experiences of sexual violence. § Draw any conclusions from your client’s decision to not report her experiences, speak of them to anyone, or pursue prosecution. |
Domestic Violence: Myths and Misperceptions
This section will break down some common misperceptions relating to intimate partner violence, often called “domestic violence.”[229] Domestic violence refers to abuse that occurs between people in or formerly in an intimate partnership. An “intimate partnership” refers to spouses, boyfriends, girlfriends, lovers, and other forms of intimate attachment. Domestic violence can occur between people of any gender. Domestic violence is like no other crime because of where it happens and from whom it stems. Our homes and our families are supposed to be places of safety. For many women, however, home is the most dangerous place they can be. Domestic violence is an umbrella term that refers to a range of actions taken by one partner against the other. It can include physical and sexual abuse, isolation, intimidation, verbal threats, emotional manipulation, and economic abuse. Control is a critical motivating factor behind domestic abuse: one partner strives to restrain the liberty of the other partner and conform their behavior to the dominant partner’s expectations. The Power and Control Wheel is a tool that illustrates the experience of being abused, and the control that an abuser exerts over a victim’s life:
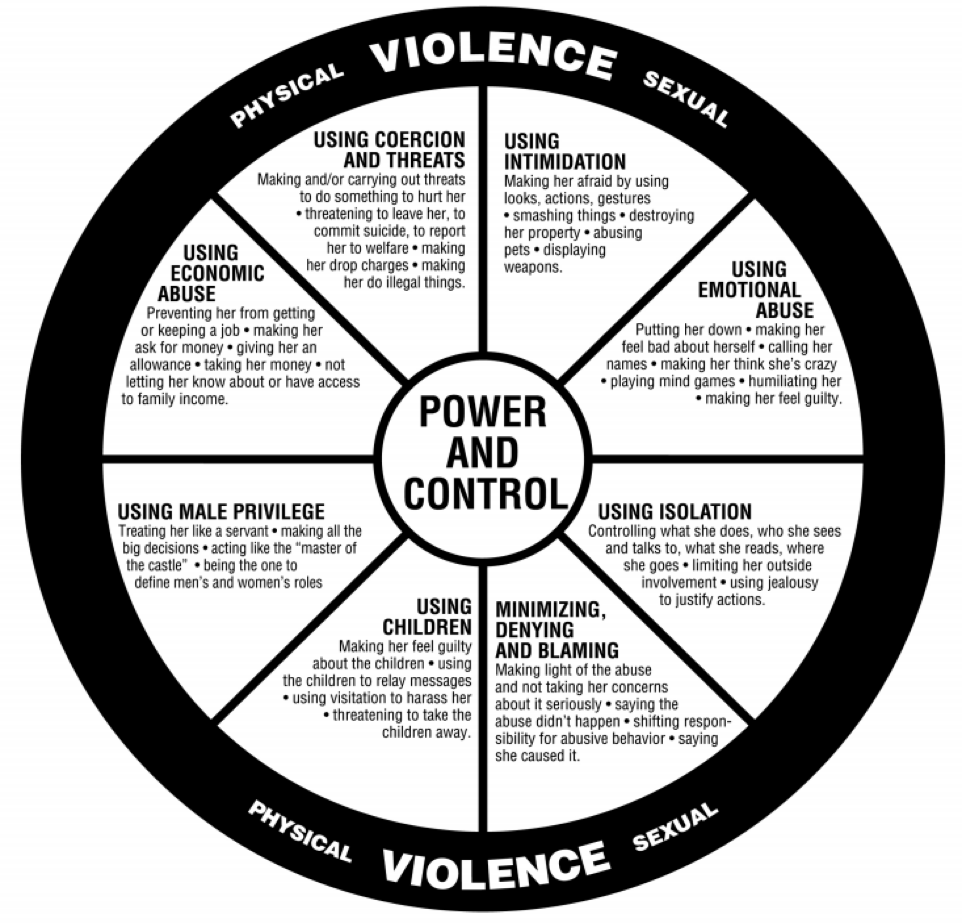
Source: coercivecontrolcollective.org
The Wheel sets forth the range of behaviors that are used to obtain power and control over a partner. It situates the physical and sexual abuse that women experience within a broader context of controlling behaviors and stresses the intentionality of those mutually reinforcing behaviors.[230] As discussed below, physical and sexual abuse are not the sole forms of domestic abuse. Domestic abuse is a prevalent threat to women all over the world over. In 2017 alone, 50,000 women around the world were killed by their partner or a family member.[231] And at 85%, the overwhelming majority of victims of domestic violence are women and girls.[232] Women experience domestic violence at all ages—sometimes when they are barely teenagers—and victims of domestic violence tend to experience multiple forms of abuse.[233] And women with multiple marginalized identities, such as LGBTQ+ women and women of color, experience disproportionately high rates of domestic violence. For example, “domestic violence within LGB relationships is twice as prevalent as in heterosexual relationships” and “fifty percent of trans respondents stated that they had been assaulted or raped by a partner.”[234] Transgender people are uniquely vulnerable to domestic violence due to “social and legal rules governing gender identity [that] contribute to an abuser’s ability to isolate [their] victim,” as well as “conscious and unconscious transphobia of service providers.”[235]
“What happens in the home stays in the home”
Domestic violence occurs within families. There is a tendency to think that as a result, domestic violence is solely a family affair. Many cultures regard the home as within a person’s sphere of privacy, a space that outsiders should not interfere with. Legal systems have reinforced this notion. In many countries, criminal law has been loath to intervene in what are largely seen as private family disputes. In some jurisdictions, police officers have been trained not to make arrests in cases of domestic violence because disputes are seen as personal.[236] Violence against women can occur in public and private spaces, and when women experience violence in the home, we must recognize those experiences and the harm they cause. Many jurisdictions now recognize that intimate partner violence is an area for public policy and government action, and international human rights law explicitly instructs states to take preventative action to protect women from domestic violence.[237] If your client has experienced domestic violence, you must be able to speak about it with her. You should not avoid discussing abuse merely because it happened in her home. Nor should you treat her experiences as any less severe because the perpetrator is her partner or former partner.
“She suffered no physical harm, so it is not domestic violence”
It is easy to conceive of domestic violence as beatings and rape. The effects of physical violence are often clear to see and the concept of sexual violence is commonly understood. The law in many countries follows this view of domestic violence, focusing on actual and threatened incidents of physical harm by one partner against another. But what about when a woman has not been physically harmed? In as many as 20% of relationships where domestic violence is present, there is no physical abuse at all.[238] Such non-physical harm can include psychological or emotional abuse, economic abuse, and coercive control. Psychological abuse is very common in situations of domestic violence. Definitions of psychological abuse vary among experts; it can be verbal but can also involve actions intended to threaten or control the victim. American sociologist Richard Tolman has developed a publicly-available tool to help understand women’s experiences of psychological abuse, the Psychological Maltreatment of Women Inventory (PMWI). This tool asks women to indicate the frequency with which certain actions have occurred in their domestic relationships. The PMWI includes statements such as “My partner treated me like I was stupid,” “My partner withheld affection from me” and “My partner put down my physical appearance.” All of these actions can contribute to psychological violence. Many victims of abuse find psychological abuse to be the most harmful aspect of domestic violence. Economic abuse is another form of domestic violence. Economic abuse refers to tactics that control a woman’s ability to acquire, use, and maintain economic resources, thus threatening her economic security and independence.[239] A perpetrator’s actions constituting economic abuse might include cutting off a partner’s access to money to pay for her daily needs, requiring a partner to request financial disbursements in order to pay for her or their children’s needs, or preventing a partner from working and having her own income source. When a woman lacks economic security and financial independence, it is difficult for her to leave an abusive relationship or develop the financial literacy she needs to survive. Control is a critical motivating factor in the abuse of domestic partners. The concept of coercive control refers to the constellation of behaviors an abuser uses to restrain a partner’s liberty and monitor her behavior. People often achieve control of their partners through non-physical means, such as intimidation, surveillance, degradation, shaming, and isolation. Intimidation is used to instill fear, secrecy, dependence, compliance, and loyalty in a victim by robbing her of psychological strength.[240] Surveillance deprives the woman of privacy and isolates her from her family, friends, and sources of support.[241] Degradation denies women self-respect, and can include behaviors such as forcing a woman humiliate herself (particularly around sex or basic bodily functions), or branding her with tattoos, burns, or bites.[242] Isolation prevents women from disclosing their partner’s behavior and from seeking help or support. Look out for indicators of each of these factors when exploring your client’s familial background. Be alert for signs that a woman’s partner micromanages her everyday life.
“Why doesn’t she leave?”
One of the most asked questions of domestic abuse victims is “why didn’t you leave?” This common reaction is natural in many ways; our instincts are to run away from harm and we cannot conceive of someone voluntarily staying in harm’s way. This question also stems, however, from a deep misunderstanding of the dynamics of domestic violence. There are many reasons why a woman might choose to stay in an abusive relationship. Just because she stays does not mean that she likes the abuse or that it can’t be that bad. Many women do not leave because they know it will be more dangerous for them if they do. As dangerous as it is in an abusive home, it is almost always more dangerous to leave.[243] The majority of domestic homicides occur while the victim is trying to leave their abuser.[244] Other reasons why a victim of domestic violence may choose to stay with her abuser include fear, a belief that her partner will change, low self-esteem, stigma about leaving the relationship—particularly in cultures that look down on marital separations—and a lack of financial resources to manage on her own.[245] Some women choose not to leave because of the children they share with the abuser, fearing that the children may come to harm, or that she will not be able to support them on her own. Even if a woman wants to leave, she is not always able to. Low-income women, for example, often lack the economic resources—such as stable housing, work, childcare, and independent income—necessary to leave a violent relationship.[246] Similarly, some women are so geographically or socially isolated that they are unaware of or unable to access support services for women leaving abusive relationships. Trans women may “feel even more dependent on her abuser for economic support” due to heightened workplace and housing discrimination.[247] Be sure to explore all factors that precluded your client from leaving the relationship, as they will be important to explain to the judge and/or jury why she stayed.
| Dos: | Don’ts: |
| § Educate yourself on the many forms of domestic violence. § Remember that domestic abuse is not always physical. § Look out for indicators of controlling behavior by your client’s intimate partner. § Engage with a domestic violence expert to inform your discussions with your client. § Look for resources for your client; she may still experience the effects of domestic abuse. | § Assume that domestic violence cannot happen in same-sex relationships. § Avoid speaking about domestic abuse because it is within a family. § Draw conclusions from your client’s decision to stay in an abusive home. |
Interviewing Your Client About Gender-Based Violence
Interviews with survivors of gender-based violence require particular care and sensitivity to earn a client’s trust, minimize discomfort, and avoid re-traumatization. This section provides an overview of effective interview techniques to elicit necessary information for a comprehensive mitigation investigation while honoring the dignity and comfort of your client. It provides considerations for each phase of the interview, namely (i) preparation, (ii) conducting the interview, and (iii) aftercare. We have drawn on the expertise of several organizations in drafting this chapter, including the Rape, Abuse, & Incest National Network (“RAINN”), WITNESS, and the Sexual Violence Research Initiative (“SVRI”). At the end of this chapter, we provide excerpts from the protocols developed by some of these organizations for additional guidance.[248]
Pre-Interview Protocol
Do Your Homework
By reading this manual, you have taken the first step in preparing for an interview with a survivor of gender-based violence: sensitizing yourself to the issue, including its causes, dynamics, and health impacts. The more you understand gender-based violence, the more likely you are to avoid perpetuating harm to victims. It is ultimately your job to educate the court about gender-based violence and how it has affected your client. Beyond sensitization to the topic, it is important to familiarize yourself with your client’s social background. The purpose of considering community or cultural context is not to generalize or shape an interviewee’s account to conform with a particular narrative, but to be an informed listener. Your client’s stories, word choice, and responses to violence may not make sense without consideration of the broader cultural context. Before or during the interview, consider the forms of gender-based violence that commonly occur in the community, how members perceive these acts, and the words used to describe them. It is helpful to recognize community attitudes towards those who have survived sexual violence and those who have committed sexual violence. In many communities around the world, for example, domestic violence is tolerated or even condoned, and victims may have internalized this community acceptance. Thus, victims may characterize violence from their intimate partner as a “quarrel,” or “discipline,” or even as a sign of affection. As we have noted throughout this manual, you must be aware of your own biases in this regard, and work to overcome them. Understanding religious or traditional practices or beliefs, the degree of women participation in community decision-making, roles and opportunities for men, women, and children in school and in the community, traditional roles in the household, status and opportunities for empowerment, and the degree of community-based systems for protection and other services and the participation of women in these systems will also help you better understand your client’s narrative.[249] For example, people often wonder why women don’t flee an abusive relationship, but if they are economically dependent on their partner—or if their partner would retain custody of their children—they may have no option but to remain.
| Dos: | Don’ts: |
| § Educate and train yourself on GBV. § Understand your client’s background. § Consider community attitudes towards persons who have survived sexual violence and persons who have committed sexual violence. § Learn about religious or traditional practices or beliefs. § Recognize societal norms regarding women and their role. § Explore whether services or protections for women exist. § Ask your client about her community and culture. § Be aware of your own biases | § Make assumptions or generalizations about your client’s experiences or community. |
Location, Privacy, and Safety
Before beginning any interview, it is critical to ensure your client’s privacy and safety. The best practice is to interview your client one-on-one and face-to-face. It is important to interview your client in-person because you can ensure that the conversation is private and that your client is in a safe space (discussed in more detail below). If you speak to your client over the phone, you have no way to ensure that the phone calls are not being monitored (particularly if your client is incarcerated) or overheard (by family members, employers, inmates, prison staff, and anyone else who may be around your client). Aside from privacy concerns, rapport and trust are best developed in person so that a client can respond to your facial expressions and body language and you can respond to theirs. Finally, interviews should be done in person so that you can assess and document critical observations about the client, including eye contact, affect, mood, facial expressions, body language, hygiene (all of which may inform mental health assessments) as well as observations about her environment, including care, treatment, conditions of confinement (if incarcerated), and housing (if not incarcerated), such as how many individuals the client is living with, the layout of your client’s living conditions, cleanliness, etc. Therefore, while phone calls and letters are a good way to stay in touch with your client about non-case-related topics, any sensitive interviews should be conducted in person. You should also interview your client one-on-one and in a safe space. Often, women with the least privacy or most reluctance to speak are the most vulnerable.[250] In prison, guards and others may have abused your client. Outside the prison context, family members, friends, and other community members may have abused her. Furthermore, your client may not be willing or able to share sensitive information in front of friends, family, employers, neighbors, prisoners, or others with whom she may have complicated dynamics, even if they are not abusive. In order to overcome barriers of shame, stigma, and familial and cultural pressures, it is necessary to interview your client in an environment of intimacy, confidentiality, and privacy. By doing so, you can shield your client from punishment and retribution and create conditions that foster trust and encourage disclosure of sensitive information. In the prison context, for example, staff may work with you to ensure you have more privacy if you explain that you will be discussing matters involving your client’s health and intimate experiences. Assure your client that you are obligated by attorney-client privilege not to share her experiences with others, and that you will discuss it with her first before disclosing any information to the court. Often, survivors of gender-based violence struggle to recount their stories to people of the same gender as their abuser. It is important to ask your client whether she prefers to speak to someone of another gender. If possible, have someone of her preferred gender conduct the interview. If this is not possible, consider having a member of the preferred gender present during the interview.[251]
| Dos: | Don’ts: |
| § Interview your client one-on-one and face-to-face. § Take your client to a private location. § If no private location is available (i.e., during a prison visit), request temporary privacy from people in the area. § Use general statements to introduce the subject matter of interviews. Consider explaining the interview topic with general statements such as “women’s health or life experiences.”[252]§ If your client prefers to speak to someone of a different gender, let another person conduct the interview. If impossible, have someone of that gender present during the interview. § Prioritize your client’s safety over the investigation. | § Reveal the subject matter or details of the interview to others. § Do not ask questions about the client’s abuse in front of others. |
Informed Consent
At the start of an interview, it is necessary that your client understands and consents to the scope of the conversation. Introducing yourself, any person that is present during the interview, your affiliations, and the purpose and scope of the interview are essential to gain your client’s trust. Explain to your client that the interview may touch on sensitive topics, including sexual relations and abuse. Explain why it is important for her defense team to understand these issues. To ensure your client understands the purpose of the interview, ask your client, in their own words, to describe its scope and purpose. Explain to your client that she can withdraw her consent at any time and choose to stop speaking. Choosing a “safe word” or a gesture that pauses or ends the interview may empower an uncomfortable or distressed client to communicate her discomfort in the moment.[253] Another helpful tool is to carry a “comfort kit”: bringing tissues, snacks, water, and a small mirror may help a client collect herself after a moment of heightened emotions.[254]
| Dos: | Don’ts: |
| § Introduce everyone in the room. § Explain the purpose and scope of the interview. Give a brief roadmap of the conversation. § Allow your client to withdraw consent or end the interview. § Choose a safe word or non-verbal cue to pause the interview. § Provide tissues, water, and other care items for your client. | § Mislead your client about the purpose of the interview. § Pressure your client into speaking about a particular issue. |
Building Rapport
Introductions
To earn a client’s trust, you must build rapport with your client. Give your client your preferred name or nickname and ask your client what name she goes by. There are many reasons that your client may not use her government name, including religious conversion, complex family dynamics, or simply that a nickname conveys a level of familiarity and care and concern. Keep in mind that your client may also identify as LGBTQ+ and may use a different name or pronouns than those associated with sex assigned at birth. In addition to asking what name your client uses, you may also want to ask what pronouns your client uses. If that is inappropriate due to cultural context (and not only your own discomfort), you can nevertheless create a safe space for someone to later disclose their sexual orientation, gender identity, and name and pronouns by doing one or more of the following: (1) introduce yourself with your own pronouns, indicating that you do not make assumptions regarding pronouns simply based on appearance or sex assigned at birth; (2) ask a more general question such as “How would you like me to refer to you?” so that the client may share what they are comfortable with; or (3) avoid using pronouns until the client self-identifies with a certain set of pronouns (he/his or she/hers). Example: “Hi, my name is Jessica and I use she/her pronouns. [If appropriate: What pronouns do you use?]”
Rapport-Building Conversation
Before delving into sensitive topics, engage your client in light conversation. Depending on where you are or the time of year, you might want to ask your client different questions: For example, can you tell me about one of the happiest moments in your childhood? What was your favorite story as a child? Did you ever have any pet animals? What crops grow in your village? What helps you pass the time in detention? You can also share information about yourself, including whether you have children, what hobbies you enjoy, and other things that will establish a relationship of trust. Regardless of the conversation topic, you want to help your client feel comfortable talking to you.
Labels
As your relationship with your client progresses and you begin to broach more sensitive topics, including abuse, be careful not to inadvertently label your client with terms such as “survivor” or “victim,” with which she may or may not identify. Pay attention to the ways in which she describes herself and what terms she identifies with and reflect that language when possible. This demonstrates that you are listening and that you are respecting her own agency to define her experiences and her identity in relation to those experiences. Similarly, avoid characterizing and labeling your client’s experiences for her. For example, your client may or may not qualify certain experiences as “rape” or “abuse” and phrasing questions with those terms may narrow the information your client provides based on their own perceptions of whether their experiences “qualify” as such. As you develop rapport, however, you can explore with your client her own perceptions of her experiences and how that fits into her worldview. In other words, you can discuss with your client how she feels about terms such as survivor, victim, rape, abuse, and why.
| Dos: | Don’ts: |
| § Introduce yourself. Go by a nickname if you have one. § Ask your client what she wants to be called. § Be friendly. Establish rapport and build trust. § Learn about your client’s life. | § Rush into sensitive topics. § Call your client a name or descriptor she does not identify with. |
Interview Protocol
Crafting Interview Questions
The following section will provide further considerations to help you craft your own questions and begin your interview. Included in an appendix to this manual is also an interview protocol document that provides sample questions and a framework for discussing gender-based violence with a client.
Framing
When crafting questions, it is helpful to consider their logical order and flow. Frequently, questions and topics are organized chronologically and thematically. For example, when speaking with a client about their experiences with gender-based violence, you may often choose to start at the beginning of her life: what was the relationship like between your parents? How did your parents discipline you? Can you describe your first sexual experience for me? What was it like for you? It is helpful to group questions by certain periods in the client’s life, or by certain experiences. For example, categories may include childhood, marriage, “before the alleged incident,” and others. If you feel you are not getting the necessary details, try returning to the topic at another time in the conversation, or try rephrasing the question. One helpful interviewing technique is “looping,” in which the interviewer asks questions that allow the client to respond broadly, but then the interviewer goes back and revisits each highlight of the interviewee’s initial response, funneling into more and more detail of each individual topic until it is exhausted. It is also important to maintain a timeline of events. If the client is unable to remember her age at the time of an event, try using other life markers or milestones: were you in school during this time? Had you begun menstruating? Was your mother still alive? As mentioned, your questions list is not a script; the interview should be conversational and organic rather than interrogatory. Truly listen to your client’s responses and ask the appropriate, organic next question. If your client shares a painful story, don’t feel as though you need to immediately move along to the next question—it is important to have a human response, whether that be to offer comfort in the form of an empathetic comment or compassionate silence. These moments are opportunities for real connection and rapport-building. At the same time, you want to make sure you are obtaining the necessary information. If your time is limited, highlight the questions that are the most important in advance and prioritize them.[255] Once you and your client have developed rapport, another useful interviewing technique is “day in the life” interviewing. This type of interview prompts your client to tell you, in minute detail, about a day in her life during a certain time period. You may want to do this for each address, or perhaps for each stage of her life (e.g., early childhood, late childhood, pre-adolescence, adolescence, etc.). In this interview, your client will be prompted to begin the story when she wakes up. Questions may include: Where are you sleeping? Who is in the room? Describe the room (sights, smells, touch). The story may continue with: what do you do after waking up? The client will take you through breakfast (if she had breakfast), morning chores, getting ready for school (if the client went to school), and every event through the end of the day, when she goes to sleep. You want to get a feel for the day; you want to be able to envision the home, the school, and all the characters in the scene. You want to understand your client’s feelings throughout the day. This interviewing technique is effective because it frequently creates the space for your client to talk about abusive experiences in an in-depth way (e.g., the client may talk about abuse at school, abuse when she returns home before other family members, etc.). It may also alert you to other witnesses who were around when the abuse occurred and provide visuals of what that abuse looked like. In a similar vein, it is also helpful to use visual imagery and/or aids to prompt memories and stories. For example, you may prompt the client to describe, in detail, their home, including the colors, the decor, the room(s), the smells, or you may prompt your client to describe their community or school. You may use photographs of the community, home, or family members to prompt detailed descriptions. Ultimately, you want to elicit a detailed narrative that will convey your client’s humanity in a real, tangible way.
| Dos: | Don’ts: |
| § Craft a logical flow to your questions. § Consider events of GBV at every stage of the client’s life. § Use “day in the life” interviewing to help paint an accurate picture of your client’s life. § Use visual imagery or aids to prompt memories and stories. § Plan to prioritize the essential questions. | § Fear deviation from your questions. § Badger the client for an answer or more detail. |
Terminology
Word choice is key when crafting your interview questions. Because people often have different notions about gender-based violence, sexual intimacy, and emotional, psychological, and physical violence, you and your client may understand the same word to have a different meaning. For example, “rape” is not strictly “sex.”[256] A client may avoid using the word rape to describe an intimate experience as sexual violence. Consider using phrases like “sexual experience” or “physical intimacy” to avoid confusion. Words like “threatened,” “forced,” “hit,” or “pushed” may also hold different meanings for different women. It is essential to be as specific and descriptive as possible: when you say, “He hit you,” what did that look like? Did he use his fists? Where did his fists make contact? Asking general questions like, “Did he sexually abuse you?” or “Did he physically or emotionally abuse you?” may not elicit the answers you want. Explain through your questions what sexual abuse or physical abuse entails: did he ever call you any names or insult you? Did he ever break or destroy your things? Did he ever control who you could see outside of the home? Did he demand physical intimacy when you did not want it? What did your arguments look like? What did he say to you? During the attack, where were his hands? Where were your hands? By eliciting specific details, you will not only avoid confusion surrounding certain terms, but you will also gain a much better understanding of your client’s experiences and be able to develop a more vivid and compelling narrative. Once you agree on the meaning of a word, you can use that word with that client if it helps the client discuss the experience. These principles equally apply when working with LGBTQ+ clients. Many individuals may not, at first, openly identify as LGBTQ+ due to cultural barriers, shame, institutional oppression, interpersonal violence, or fear of that information being shared with others. Still other individuals may never use the language of “lesbian, gay, bisexual, transgender,” but may describe same-sex sexual or romantic relationships and gender non-conforming identities and expressions. It is important to always create space for someone to disclose these parts of their experience and identity, rather than force disclosure, and to respect each individual’s right to self-determine their own identity. If your client has had same-sex relationships, but does not identify as gay or lesbian, you should respect that. If your client was previously in a heterosexual marriage, but now identifies as lesbian, you must respect that as well. Use the words that you hear your client using, and as your relationship progresses, you can have conversations about how your client’s identities have shaped their lived experiences, including their experience of incarceration. Importantly, you cannot tell by someone’s appearance whether they identify as LGBTQ+, so do not presume that your client does or does not identify as heterosexual, cisgender, or any other identity. That means that you should not ask questions that presume your female-identified client had a “boyfriend,” rather than another gender-ed partner; that your client who was assigned female at birth in fact identifies as female (or that a client assigned male at birth in fact identifies as male); or what “sex” means.
| Dos: | Don’ts: |
| Do say: “Tell me about your first romantic experience.” | Don’t say: “Tell me about your first boyfriend.” |
Avoiding presumptions of what “sex” means is not only important when working with LGBTQ+ clients, but with all individuals. The prevailing concept of what constitutes sex is defined by heterosexual norms, but many individuals have sex without penetration or emphasis on reproduction. Additionally, many individuals who have experienced sexual abuse may not incorporate those experiences into their narrative of their own sexual experiences and journey. For example, someone who was raped as a child or molested by a parent may not consider that assault their “first sexual experience.” That does not mean you cannot ask about your client’s first sexual experience—indeed, you should do so—but it does mean that you cannot preclude prior sexual experiences that your client may hold in a separate category. Simply put, always keep an open mind and avoid tunnel vision. It is important to respect your client’s agency and allow her to be the narrator of her own story. You can create the space for this by avoiding “shortcut” terminology that does not allow for explanation, challenging your own assumptions about the definitions of sex, and not inserting those assumptions into your questions. Don’t say: “Tell me about when you lost your virginity.” This is an example of a “shortcut” word that means different things to different people and may inhibit a client from sharing experiences of sexual abuse or may narrow the response of an LGBTQ+ client.
| Dos: | Don’ts: |
| § Ask for clarifications on word meaning. § Ask specific and descriptive questions. § Ask follow-up questions to learn details. | § Shy away from difficult or uncomfortable topics. § Use words like “rape,” “sexual abuse,” or other general phrases to describe experiences. § Assume you and your client agree on the meaning of a word or phrase. § Assume your client’s sexual orientation or gender identity. § Use shortcut terminology. |
Question Form
In order to elicit the most information, detail, and imagery, it is important to ask open-ended questions. These questions typically begin with the words “who,” “what,” “when,” “where,” and “how.” The answers to questions phrased in this way will result in much more information than questions that call for a yes or no response, such as those beginning with “do” or “did.” Sometimes, a question isn’t necessary at all, and you can use prompts, such as: “tell me more about [x],” “describe [x],” “please explain,” or “give me an example of [x].” Allowing for silence may also result in the client speaking up and providing more information, as can simply providing empathetic and validating responses, such as, “That sounds really difficult,” or “I’m sorry that you experienced that.” All of these approaches create space for your client to continue sharing more information. While it is important to start with broad, open-ended questions, as the conversation progresses and you explore an individual topic in-depth, you can narrow your questions to prompt more detail about certain points and/or stories. This is sometimes referred to as a “funnel approach,” in which questions first cast a wide net and slowly hone in on more specific information. If you start with narrow questions, you will never know the universe of information; on the other hand, if you never narrow down your questions over the course of a conversation, you may not elicit the level of detail needed to develop vivid imagery and compelling vignettes, such as smells, sounds, textures, tastes, and descriptions of a person, place, or experience that humanize your client to the decisionmaker. It is especially important that your questions respect the comfort and dignity of your client. Do not imply the interviewee could have avoided or prevented the situation. Consider whether a question may come off as rude, offensive, or shaming. Do not ask questions to intentionally provoke emotional responses or obtain guarded information. Appreciate that people recount trauma differently; avoid making assumptions about your client’s tone. Recognize that memory lapses or contradictions in storytelling are symptoms of trauma. Do not ask questions that doubt the truth of the narrative. Avoid reinforcing false and harmful narratives about gender-based violence, including that abuse is inevitable and survivors are blameworthy. Your goal is to display empathy and compassion, and your questions should ultimately be asked in a factual, non-judgmental way. Avoid questions that begin with the phrases “why did you” or “why didn’t you;” such questions tend to suggest blame or judgement: Why did you go alone? Why don’t you know who raped you? Why didn’t you tell anyone? Why didn’t you call the police? Why didn’t you leave? Why didn’t you say no? What were you wearing when you were raped? Instead, consider asking questions that allow the client to explain herself in a non-defensive way: Can you tell me about the events before/during/after the attack? When X happened, what were you feeling? How was this experience different from other intimate experiences you have had? Was there someone you felt comfortable talking to at the time of the event? What are your hopes for the future? Is there anything else you would like to add?[257] Finally, be aware of your own discomfort in talking about very sensitive, painful topics and ensure that your discomfort is not driving the interview. For example, if your client is opening up about an experience of sexual abuse, do not allow your own discomfort to cut the conversation short and move on to the next topic as soon as you hear the initial description. This is something that many of us do without even realizing it. It is important that you sit with the client in her story, elicit the important details that you need, and be emotionally available.
| Dos: | Don’ts: |
| § Ask open-ended questions. § Ask questions rooted in compassion and understanding: “what did you feel when . . . .” § Ask factual, non-judgmental questions. | § Ask “yes or no” questions. § Ask questions that indicate blame or shame: “why didn’t you. . . .” § Question the truth of the narrative. § Ask provocative, highly emotional questions. § Make assumptions based on your client’s tone or demeanor. |
Behavioral Considerations
Your behavior during the interview is equally, if not more, important than the questions you ask. While your question list should serve as a guide, it should not be a script. Adjust your questions to allow for a more natural flow of conversation. Minimize your amount of notetaking; if necessary, limit your notes to points for follow up. Your priority should be to help your client feel comfortable and heard. (You will, however, need to write up your notes as comprehensively as possible within 48 hours of the interview so as not to forget any information. It is vital that you preserve the client’s memories and words, as you do not want to unnecessarily re-traumatize her by repeating questions in later interviews.) It is necessary to engage in active listening. Stay silent while your client speaks. Do not interject with phrases like “yes,” “mm-hmm,” or other noises that may disrupt the flow of the interviewee’s story. Use eye-contact, head-nods, or other non-verbal gestures to indicate active listening.[258] Maintain open body language by sitting square with your client and removing physical barriers. Ensure that others present during the interview do the same. Be patient. A survivor may take time to recount a story. Due to trauma, survivors may tell stories that have gaps or miss essential details. If necessary, go back to uncover essential information, but do not pressure the interviewee. Avoid showing discomfort, shock, or horror during the interview.[259] This may make the interviewee feel uncomfortable or embarrassed. You can communicate empathy by actively listening, providing a tissue if the client needs it, and by telling her you are sorry for what happened to her. Avoid touching your client, as this could trigger a flashback—particularly if you are the same gender as her abuser. While paraphrasing is a helpful technique to signal to your client that you are carefully listening, avoid over paraphrasing or careless paraphrasing. Such paraphrasing may come off as minimizing or generalizing a survivor’s experience. Similarly, assuming how a survivor feels about an experience or how she should have acted can be equally harmful. Avoid giving advice or suggesting a course of action. Instead of saying phrases like, “you should report” or “you should find a therapist,” consider supportive language like, “Would you be interested in resources that may help with healing and recovery?” Using language of validation and support throughout the interview may also help comfort your client. After a client communicates a difficult experience, consider thanking them for sharing it, acknowledging how difficult the experience must have been for the client, and apologizing that the experience happened.[260] If the interviewee becomes distressed, respect the interviewee’s boundaries. Immediately offer to stop if she is uncomfortable, tired, or asks for a break. If an interviewee cries or becomes emotional, pause the interview and give her time to regain composure.[261] Offer to continue the interview at another time.[262]
| Dos: | Don’ts: |
| § Encourage the natural flow of conversation. § Maintain open body language and eye contact. § Listen silently but actively. Use non-verbal cues to indicate your attention. § Provide reassuring and validating comments. § Take minimal notes. § Stop the interview if the client becomes uncomfortable, distressed or emotional. | § Stick to the script. § Have closed body language, minimal eye contact, or a bored look. § Ignore a client’s expressions of fear or discomfort. § Interrupt your client. § Rush a story. § Question gaps in the narrative or demand proof. § Show shock or horror during the interview. § Over-paraphrase. § Make assumptions about how a client feels about the experience. § Suggest a course of action. § Pressure a distressed client to continue the interview. |
Working with Translators
As a threshold matter, it is important to ensure your selected translator is trustworthy and qualified. Where possible, consider taking recommendations for translators from NGOs and other professionals who use them frequently to discuss gender-based violence or other sensitive topics. Once you select a translator, the same behavioral considerations for the interviewer pertain to that person. Before the interview, you should meet with the translator to share and review questions, agree on terminology, and discuss any security considerations. It is important that you discuss proper translations and connotations for key words and phrases before the interview to avoid confusion or miscommunication. If the client has expressed a preference for an interviewer of a particular gender, you should consider whether she may also prefer a translator of a particular gender. Remind the translator not to speak over the interviewee and to wait a few seconds after the interviewee speaks to begin translating.[263] Explain to the translator that their reactions and body languages are equally important to ensure the comfort of the client.
Working With Untrained Interpreters: A Cautionary Tale
Several years ago now, I sent a student to interview Alice Nungu, a woman in Malawi who had been sentenced to death. We knew that Alice had been in a violent marriage, but we knew very few details. When we arrived at the prison, we met with our interpreter—a paralegal named John (not his real name) who worked with a local NGO. My student was very well prepared for the interview, and had received training in trauma-sensitive interviewing. The team left to conduct the interview together. When my student returned from the interview, she was very upset and asked to speak to me. She told me that when she asked Alice, “Can you tell me about a time when your husband was violent with you?,” the interpreter got up, mimicked boxing, and interpreted the question while boxing and laughing. Alice did not laugh, and my student was horrified. We never worked with that interpreter again, and luckily he did not do any lasting damage. It was a lesson to me that we must train our interpreters as well as we train lawyers and investigators, as their tone, body language, and demeanor is crucial to establishing a relationship of trust and respect with our clients.
| Dos: | Don’ts: |
| § Select a trusted and qualified translator. § Share your questions with the translator in advance. § Agree on terminology. § Discuss security concerns. § Consider that the interviewee may prefer a translator of a particular gender. § Ensure the translator treats the client with respect. | § Allow the translator to interrupt the client. § Have side conversations with the translator in front of the client during the interview. |
Post-Interview Protocol
Aftercare
Interviews regarding gender-based violence are prone to leaving your client feeling emotionally fragile, vulnerable, or upset. It is important to ensure that you leave your client in a good place physically and emotionally. One way to help your client is to ask if she would like to continue the conversation: Are there any other experiences you would like to share? Is there anything else you think we should talk about? By giving your client space to speak, she can share thoughts and feelings that may still loom in her mind. Remember to offer items from your “comfort kit”: tissues, snacks, water, and a small mirror may help a client collect herself after a moment of heightened emotions. Sometimes, breathing exercises or meditations can help a client return to a more relaxed state.[264] Easing back into casual conversation by asking lighthearted questions, like those used to build rapport at the beginning of the interview, may help bring the client back to a calm place. If there is an activity your client likes doing to ease their tension, invite them to partake in that activity. Clients may have questions or concerns about how the information they provide will be used for their case. It is important to make space for these questions. Proactively take the time to explain again how you will use the information, why it is important, and what the next steps of the case will be. Offer to provide information about mental health, substance abuse, or other applicable services if you think your client may have an interest in them.[265]
| Dos: | Don’ts: |
| § Ask your client if she would like to share any other experiences. § Remember to offer tissues, water, and other care items for your client. § Consider breathing exercises or meditation to ease a troubled client. § Return to light-hearted conversation before ending the discussion. § Let your client choose the form of aftercare that works best for her. § Provide information to your client about next steps in the case. § Offer information on services to support your client. | § End the interview abruptly or immediately after serious discussion. § Leave the client in a distressed state. § Force any one form of aftercare for your client. § Insist on psychological or other forms of support against your client’s wishes. § Leave your client in the dark about her case. |
“Who amongst us is willing to sit before strangers and our mothers and children, and relive the worst moments of our past—even if it means a much lower sentence? Nobody likes to be pitied and nobody wants their children to see them as damaged.” —Kwaneta Harris, currently incarcerated.
Concluding Remarks
Interviewing a client about her experiences with gender-based violence is no simple task: it takes careful planning, active listening, patience, and compassion. Despite its difficulties, a conversation about gender-based violence is critical for a full mitigation investigation and proper representation of your client. Often, you will be the first person that your client speaks to about her experiences of abuse. By planning open-ended, specific, and empathetic questions and displaying care and concern for your client before, during, and after the interview, you can have a conversation that leads you to the right information and leaves your client feeling supported.
Chapter 5: Treatment of Women in the Criminal Legal System
“As a black female who has suffered through different types of trauma and violence, it is very hard to be incarcerated in a system that continues to abuse me and disregard my needs.” —Erica Sheppard, incarcerated on death row. This chapter focuses on how gender affects women’s interactions with police, prosecutors, courts, and co-defendants. We also highlight the myriad ways that women can experience discrimination on the basis of multiple identities. Understanding these intersecting forms of discrimination is vital when defending women who are members of minority groups, foreign nationals, disabled, or gender nonconforming. Much of this chapter draws from previous publications of the Cornell Center on the Death Penalty Worldwide, including Judged for More Than Her Crime: A Global Overview of Women Facing the Death Penalty and No One Believed Me: A Global Overview of Women Facing the Death Penalty for Drug Offenses. Both publications are available at www.deathpenaltyworldwide.org/publications/.
Women and Police Interrogations
Women—particularly gender nonconforming women and women from minority cultures—are vulnerable to sexual abuse, harassment, and coercive interrogations by law enforcement. In the United States and around the world, police sexual violence against women is “widespread, underreported, and under addressed.”[266] Women are most vulnerable when they are alone in police custody, before they have access to the courts or legal counsel. There, police may wield their power to extort sexual favors, intimidate women into confessing, or simply exploit the vulnerability of women who are under their control and incapable of fighting back (see Chapter 2). Many victims of police sexual violence never report the crime, either out of shame, fear of retaliation, or the sense that they will not be believed.[267]
Kanizan Bibi: A Case of Police Torture, Mental Illness, and Powerful Advocacy by Justice Project Pakistan
Kanizan Bibi is a fragile, mentally ill woman who spent more than 30 years on death row in Pakistan. Kanizan grew up as a child of poverty and was her family’s principal breadwinner beginning at age fourteen. Before her arrest, Kanizan worked as a housemaid for Khan Muhammad, a rich landowner, and his family. She spent nearly two years caring for and playing alongside her employer’s children, whom she loved dearly. Tragically, in 1989, Khan Muhammad’s wife and five children were murdered. After rumors circulated that Kanizan was having an affair with Khan, she was arrested. The police recorded Kanizan’s age as 25, though her family said she was only about 16 years old at the time. Kanizan was tortured in police custody for nearly fifteen days. The police hung her from ropes, tortured her with mice, and electrocuted her. Villagers living close to the police station said they could hear screams from the station at night. Kanizan was so badly injured that she had to be hospitalized. Eventually, under torture, Kanizan told her interrogators what they wanted to hear. Her “confession” became the centerpiece of the prosecution’s case, and she was convicted and sentenced to death. The prison was far from her family home, and her family was only able to visit her three times in 30 years. After spending years on death row, Kanizan was diagnosed with schizophrenia. She became withdrawn and was unable to speak for over a decade. She lost touch with reality and became oblivious to her surroundings. Justice Project Pakistan took on her case and launched a public campaign to raise awareness about her plight. They created a powerful video to tell her story, available at https://deathpenaltyworldwide.org/kanizan-bibi-alice-profile/. In February 2021, the Pakistan Supreme Court finally commuted her death sentence and ordered her transfer to a mental health facility where she could receive treatment for her illness. LGBTQ+ people also experience pervasive and severe police harassment and violence. Frequently, police use neutral laws as a pretext for targeting LGBTQ+ people. In April 2020, for example, Ugandan police arrested twenty-three people living in a youth shelter serving lesbian, gay, bisexual and transgender people under the guise of enforcing COVID-19 restrictions; and yet, video shows the mayor who led the raid “berating residents for ‘homosexuality,’” “beating them with a stick,” and searching the shelter for “evidence of homosexuality, which is punishable by up to life in prison.”[268] Police use other purportedly neutral laws[269] and policies, such as stop-and-frisk,[270] to disproportionately and discriminatorily target LGBTQ+ people.[271] Once arrested, LGBTQ+ people are often subjected to violence and harassment.[272] In 2019, Ugandan police arrested sixteen activists associated with an organization supporting LGBTQ+ youth, charged them with “carnal knowledge against the order of nature,” and performed forced anal examinations.”[273] In Cameroon, there have been “extensive human rights violations in arrests and prosecutions [of LGBTQ+ people], including the use of forced anal examinations and other forms of torture and ill-treatment, forced confessions, denial of access to counsel, and blatant anti-LGBTQ+ bias on the part of judges.”[274] During interrogations, police officers may also threaten to reveal a person’s sexual orientation to friends, family or colleagues to obtain a confession.[275] In the United States, police sexual violence disproportionately affects women of color—particularly Black women and girls.[276] In other countries that impose extreme sentences, there is little research on the targets of police sexual violence. It is important that you specifically ask your clients whether, at any time while they were in police custody, they were touched, insulted, or subjected to any kind of sexual overtures or innuendo. Such behavior may be criminal, and it is also directly relevant to the admissibility of any statement your client may have made to the police. Even where the police do not engage in violence or sexual harassment, women may be vulnerable to coercive police tactics. Most women who come into contact with the criminal justice system are victims of trauma—and frequently, their trauma is tied to mistreatment by men in their lives. Research shows that past trauma is associated with heightened suggestibility among individuals who falsely confess to crimes (see Chapter 3).[277] Similarly, domestic violence victims may have “automatic, often unconscious habits of obedience,” making them vulnerable to authority figures.[278] Victims of intimate partner violence are also more apt to internalize guilt. This means that victims of gender-based violence are more apt to acquiesce to aggressive questioning by police, which in turns heightens the risk that they will falsely confess to a crime they did not commit.[279]
Bias from Judges and Prosecutors
Judges and prosecutors are not immune from gender bias. As Chapter 4 notes, all lawyers fall prey to gendered stereotypes and misperceptions. You must therefore be well-equipped to defend your client from gender bias by courtroom actors. At times, women charged with crimes can benefit from gender stereotypes that characterize them as weak, submissive, and non-violent. But women charged with murder and other capital crimes are often demonized precisely because they “are perceived to have betrayed traditional gender roles.”[280] As we discuss in Chapters Four and Six, dominant societal norms dictate that women are expected to be modest, meek, and maternal. Prosecutors weaponize these gender stereotypes to condemn women for not behaving according to traditional expectations. For example, prosecutors in one U.S.-based murder case presented the defendant’s alleged shortcomings as a mother as evidence of her guilt. The same prosecutors presented multiple witnesses who testified about the defendant’s purportedly provocative clothing.[281] The use of negative gender stereotypes to attack a woman’s character or impugn guilt violates her rights under international law, we explain in Chapter 6. You must be proactive in preventing the use of such stereotypes in order to protect your client’s fair trial rights.
| Dos: |
| § File pretrial motions or applications to the court to prevent prosecutors from using your client’s deviation from traditional gender roles as evidence of her guilt or moral blameworthiness. In particular, request that the court bar the state from: o Introducing evidence of your client’s mothering abilities when it is irrelevant to her alleged crime. o Referring to your client’s gender identity or sexual orientation. o Introducing evidence of your client’s sexual history. o Introducing evidence of your client’s failure to conform to traditional female roles in her partnership or marriage. § In international tribunals, consider raising violations of your client’s right to be free from gendered stereotyping (see Chapter 6). |
Judges and jurors are also prone to evaluate women’s behavior against the yardstick of culturally dominant gender norms. In our publication Judged for More Than Her Crime, we describe a case in India where a woman was sentenced to death for killing her husband. The judge characterized her as the “kind of woman” who brings “shame” upon her family, village, and society and who represents a threat to women and men alike. Referring to the woman’s extramarital affair, the court commented that “a lady of such character deserves no leniency.”[282]
| Dos: |
| § Remember to educate the court about your client’s life circumstances, as we discuss in Chapter 4, to offset the power of negative gender stereotypes. § Object to any sexist language that a prosecutor or judge uses, particularly where it is necessary to lodge an objection to preserve the issue for appeal. |
Women with Male Co-Defendants
Women facing extreme sentences are frequently arrested together with male suspects. In India, at least nine out of 12 women on death row were charged with one male co-defendant and at least six of these men were their intimate partners.[283] Seven out of nine cases of women on death row in Indonesia also involved male co-defendants, usually an intimate partner.[284] Many women sentenced to death for drug trafficking were brought into the drug trade by male romantic partners. Yet male co-defendants or co-suspects often face lesser or no criminal consequences for their actions, even if they played a key role in the drug-related activity. Lawyers sometimes make the mistake of representing multiple defendants in the same criminal case. In most cases—and particularly in capital cases—this gives rise to a conflict of interest that violates the rights of the accused to effective legal representation. This is particularly true when you are representing a woman charged alongside a male co-defendant. It is rarely in a woman’s best interest to be tried together with a male co-defendant. The prevalence of intimate partner violence among women facing serious offenses is high, the importance of which is discussed in Chapter 4. Your client’s co-defendant may have abused her in the past, and their relationship may influence her actions and testimony during trial. For example, a woman may be unwilling to discuss the extent to which her partner abused her if he is present in the courtroom. In meetings with their defense attorney, her male co-defendant may insist on certain strategies that are not in her best interest. And in all cases, the mitigation narratives of male and female co-defendants will diverge significantly, and may put the other in a negative light.
| Dos: |
| § If you are in a jurisdiction where you are assigned to represent multiple defendants in a capital case, you should insist on their right to individual, conflict-free representation. |
Intersectional Discrimination
Throughout this manual, we refer to the intersectional forms of discrimination that women suffer. The concept of “intersectionality” refers to the fact that some people experience distinct forms of oppression that coincide to amplify the discrimination the person suffers.[285]
Women from Racial or Ethnic Minorities
Women from racial or ethnic minorities experience discrimination both because they are women and also because of their race or ethnicity.[286] The UN Committee on the Elimination of Racial Discrimination has recognized that “some forms of racial discrimination have a unique and specific impact on women” and that racial and gender discrimination are “interlinked.”[287] For example, prosecutors in the U.S. have combined racist imagery—such as implying that a Black American is an animal[288]—with gendered stereotypes to secure a conviction. Women belonging to racial or ethnic minorities may also experience further discrimination on account of their class, disability, gender identity, or other factors. Together, these forms of discrimination intersect to create additional barriers to justice.
Erica Sheppard: A Victim of Intersectional Discrimination
Erica Sheppard, a survivor of child abuse, domestic violence, and multiple rapes, was sentenced to death in the U.S. state of Texas for a crime she committed at the age of nineteen. At the time of her arrest, Erica had three children; she was homeless and mentally ill. As a young Black girl growing up in poverty, she had little social support, even after being raped and becoming pregnant as a result. At seventeen, Erica met Jerry Bryant. Throughout their two-year relationship, Bryant beat her repeatedly, held a gun to her face, and threatened to kill her. She twice went to the police for help, and each time they failed to arrest Bryant—a common response when Black women report incidents of domestic violence. Erica sought refuge at a battered women’s shelter, where she hoped to receive counseling and assistance. But the shelter would not keep her. Twenty-seven days later, she encountered a man who coerced her into participating in a robbery where he killed a woman. In court, Erica received a state-appointed lawyer who was inept, inexperienced, and had never tried a capital case. Judge Carolyn King, a federal appellate judge, described Erica’s life history as “horrific,” “traumatic,” and “abusive.” Yet the prosecution ridiculed Erica’s trauma, accusing Erica of making up the assaults: “Any bruises, any scratches? Any fear? She was not physically abused; but even if she was, what kind of excuse is that?” The prosecutor called her a “jackal” and exaggerated her role in the offense, downplaying her youth and lack of criminal record. The jury never heard about her extensive history of trauma and its impact on her mental health, and they sentenced her to death. Erica, who has now been on death row for 26 years, observes, “Using capital punishment or incarceration as the sole response to violence fails to achieve justice for all because you’re simply sending people, especially Black and brown people, into a system that’s already failed them.” As a defense lawyer, you must consider the different forms of oppression that your client faces at every step of her legal proceedings. Exploration of the historical, political, and cultural context of your client’s life must be a central component of your mitigation investigation. Educate yourself on the discrimination faced by minority racial and ethnic groups in your jurisdiction, understand how discrimination affected your client’s life prior to her offense, and use all the tools at your disposal—such as challenging peremptory strikes, if you are in the United States—to oppose discrimination based on race and gender in your client’s case. The American Bar Association’s toolkits on combating racial bias in the courtroom are a helpful resource: https://www.americanbar.org/groups/diversity/resources/implicit-bias/.
Foreign National Women
In some countries, foreign nationals—and, in particular, foreign migrant workers—are sentenced to death in disproportionate numbers. This is especially true in Gulf nations like the United Arab Emirates and Saudi Arabia, and extends to foreign women on death row, many of whom are domestic workers.[289] In the UAE, for example, of the approximately 200 people on death row, only 19 are UAE nationals. Of the nine women on death row in the UAE, eight are foreign nationals and most of them are domestic workers.[290] All migrant workers, both male and female, are particularly vulnerable to unfair capital trials: they are poor, they lack linguistic, cultural, and institutional knowledge of the criminal justice process, and they are often denied access to effective legal representation and translation.[291] In addition, language barriers, illiteracy, and economic vulnerability may leave migrant workers at particular risk of forced and false confessions.[292] Migrant workers may also be trafficking victims. It is vital that you explore the conditions under which your foreign national clients were brought to the country, the nature of their employment, and the constraints placed upon them by employers. These facts are particularly important where foreign nationals are accused of killing their employers. If they are not fluent in the language of the country where they are tried, foreign national defendants are entitled to an interpreter in every criminal process, free of charge and immediately following arrest, including during police interrogations.[293] Moreover, under well-established international law, arresting or detaining states must notify foreign nationals of their right to consular notification and access.[294] Consular representatives can provide critical assistance to their nationals facing a capital sentence abroad, such as access to a competent interpreter, assistance with gathering relevant information in the home country to bolster the defense, and sometimes support for legal aid.[295] State authorities have an obligation to contact consular officials without delay if the detained or arrested foreign national requests that they do so.[296] State compliance with this obligation, however, varies widely. If the state has failed to notify your client of her consular rights, and if your client would like to communicate with her consular representatives, you should insist that the state authorities fulfill their obligations under international law. If your client was convicted and sentenced to death without ever being notified of her rights to consular notification and access, you should argue that she is entitled to reconsideration of her conviction and sentence in accordance with the decision of the International Court of Justice in Avena and Other Mexican Nationals.[297]
LGBTQ+ People
LGBTQ+ people, and in particular transgender women, face pervasive violence and discrimination at every stage of the criminal legal process, from arrest to sentencing to incarceration. LGBTQ+ youth and adults are overrepresented in the criminal justice system worldwide.[298] As of 2020, 70 countries criminalize same-sex sexual conduct, including 38 countries that either criminalize same-sex conduct regardless of sex or explicitly criminalize sexual conduct between women.[299] Additionally, at least 13 countries have laws that prohibit people from presenting as a gender other than the gender they were assigned at birth.[300] In these countries, LGBTQ+ persons are subject to arrest and incarceration—and, in eleven countries, the death penalty—because of the criminalization of their very identity.[301] Even in countries without express criminalization of LGBTQ+ identities, relationships, and gender expression, LGBTQ+ people experience disproportionate contact with the criminal justice system. In the U.S., for example, lesbian and bisexual women are four times more likely than straight women to be arrested[302] and 47% of Black transgender people have been incarcerated at some point in their lives.[303] This high rate of contact with the criminal legal system is due to “[a] history of bias, abuse, and profiling toward LGBTQ+ people by law enforcement,” along with high rates of poverty, homelessness, and discrimination in housing (including homeless shelters) and the workplace.[304] For many LGBTQ+ people, widespread discrimination, poverty, and social stigmatization thrust them into survival economies, such as sex work, which, in turn, are criminalized. For LGBTQ+ juveniles, family rejection, homelessness, hostility in state-run homes and institutions, and discrimination in schools also push LGBTQ+ youth into the criminal legal system.[305] At trial, prosecutors will often weaponize harmful sexist, homophobic, and transphobic stereotypes to dehumanize LGBTQ+ clients and obtain the most severe penalty. For example, in the United States, the prosecutor suggested that Bernina Mata’s lesbian identity was the motive for the crime —specifically, that because Ms. Mata was such “a hard core lesbian” who “by nature loathed men,” she murdered the male victim after he made a pass at her.[306] In another U.S. case involving Wanda Allen, a Black lesbian, the prosecutor “relied on sexist, racist stereotypes regarding Ms. Allen’s butch identity and masculine appearance to defeminize, dehumanize, and prejudice her in front of the jury, thus ensuring her death sentence.”[307] Prosecutors have also used clients’ lesbian and transgender identities to diminish the severity of their punishment if incarcerated by implying that incarceration with individuals of the same sex assigned at birth would be sexually enjoyable. This argument not only mischaracterizes and misunderstands LGBTQ+ identities and relationships, but it also grossly minimizes the fact that LGBTQ+ prisoners often face physical and sexual violence and discrimination in housing, medical care, strip searches, and solitary confinement. This is described in more detail in Chapter 2 of this manual, “Conditions in Jails and Prisons: What You Need to Know.”
Women in Poverty
Many women in the criminal justice system, and the vast majority of those on death row, are from poor and marginalized communities. Many are illiterate and unaware of their legal rights. Without the resources to hire a lawyer, they are wholly dependent on state-appointed legal counsel.[308] Illiteracy and lack of education among poor women leave them more vulnerable to discrimination, coercion, and exploitation. As women in a patriarchal society, women on death row are subject to gendered systems of oppression that often push them into economic insecurity. Women disproportionately occupy part-time, low paying jobs[309] with short-term contracts or no contracts at all and little opportunity for career progression—in other words, precarious work.[310] This labor market gender segregation is partly attributable to discrimination by employers, who may be less likely to hire or promote women because they expect women to leave the labor market when they have children.[311] In most cultures, women are also responsible for providing care and financial support to both their immediate and extended family.[312] This unpaid care burden is exacerbated for single mothers, who make up the majority of one-parent households[313] and face significantly higher poverty risks than average. Single mothers must support their family on a sole income, which is often inadequate, and they often struggle to juggle paid and unpaid work. They also face additional challenges due to their gender, such as pay gaps and motherhood pay penalties.[314] Understanding the economic hardships that your client has faced will help you provide context for her actions, particularly if she is charged with a crime involving financial gain, such as burglary or robbery. It will also help you explain why she may have been under additional mental strain at the time of the crime.
Chapter 6: International Human Rights Law
This chapter will illustrate how defense teams can use human rights law to reframe clients’ narratives. It will also show how human rights law allows you to contextualize your client’s offense in the fuller fabric of her life. Often, it is difficult for judges and jurors to see women defendants as both victims and perpetrators. A human rights framework can help you overcome this challenge. For example, understanding the state’s due diligence obligations under international law will enable you to explain how the state violated its human rights obligations to your client even before she was arrested and charged with a capital crime. By so doing, you can shift the narrative of your client’s case from one that exclusively examines what she did wrong to one that highlights how the state failed her.
Human Rights Law and Women’s Death Sentences
Every major international and regional human rights treaty prohibits discrimination on the basis of sex. In addition, there are both international and regional treaties that focus on the human rights of women, such as the UN Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW); the Protocol to the African Charter on the Rights of Women in Africa (Maputo Protocol); and the European Convention on Preventing and Combatting Violence Against Women and Domestic Violence (Istanbul Convention). While these treaties do not address capital punishment, they are directly relevant to how states treat women both before their arrest, during their trials, and after their convictions and sentences are imposed. Where treaties and protocols recognize women’s rights, states have corresponding obligations to respect and protect those rights.
Using International Law: Maimuna’s Case
Maimuna was married at the age of thirteen. Five months into her marriage, her husband burned to death in an alleged arson attack while he slept. Maimuna was arrested and charged with his murder. She languished in prison for six years while her trial dragged on. In 2012, a Nigerian court convicted Maimuna of culpable homicide and sentenced her to death. Lawyers acting pro bono challenged her death sentence before a regional court, the ECOWAS Community Court of Justice, arguing that imposing a death sentence on a juvenile violated international law and the African Charter on the Rights and Welfare of the Child. The ECOWAS court ruled that Nigeria had violated its international human rights obligations, ordered a stay of execution, and awarded Maimuna damages.[315] Maimuna was released from prison in 2016.
Human Rights Restrictions on the Death Penalty
Human rights law also outlines internationally-agreed parameters for the application of the death penalty. The UN International Covenant on Civil and Political Rights (ICCPR) protects all individuals’ right to life.[316] Because the right to life is fundamental, the international community has limited the legal application of the death penalty, for example by exempting certain categories of offenders from capital punishment. Among these exempt categories are people with intellectual disabilities, people under the age of 18, and pregnant women.[317] For a helpful overview of limitations on the application of the death penalty under international law, the Cornell Center on the Death Penalty Worldwide has compiled summaries with reference to treaty provisions and relevant jurisprudence on its website at https://deathpenaltyworldwide.org/publication-categories/international-legal-issues/. International and regional human rights treaties uniformly prohibit the execution of pregnant women. Depending on the country, pregnant women who receive a death sentence either benefit from a commutation to a term of imprisonment or receive a stay of execution until after the birth of the child.[318] Once a woman under sentence of death has given birth, international jurisprudence is silent as to whether and when she can be executed, and regional jurisprudence on the issue varies widely.[319] Regional instruments such as the Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa,[320] the African Charter on the Rights and Welfare of the Child,[321] and the Arab Charter on Human Rights[322] further prohibit the execution of mothers of infants and young children,[323] while the Arab Charter prohibits the execution of any “nursing mother within two years from the date of her delivery.”[324] These exemptions are driven in large part by states’ consideration for the welfare of unborn children.[325]
| Dos: |
| § Find out if there is a possibility that your client is pregnant or if she has an infant or young child. § Be sensitive to any particular difficulties your client may face when discussing pregnancy, sex, and relationships (e.g., trauma, young age, intellectual disability). Where possible, work with a gender-sensitive specialist. See Chapters 2 and 4. § Research your jurisdiction’s standards for sentencing women with small children, where applicable. § Consider the implications of the Bangkok Rules regarding women with children in your advocacy. See Chapter 3. |
Using Human Rights Law to Reframe the Narrative
Most women facing extreme sentences were victims of human rights abuses before they were defendants. These human rights abuses, where known to the state or perpetuated by the state, trigger obligations on the part of the state to protect the victim’s human rights and to support her. The state’s obligations are known as “due diligence” obligations.
What is the due diligence framework?
All people have the right to be free from discrimination and to equality before the law, regardless of their gender. Common forms of gender-based discrimination against women include, but are not limited to: sexual abuse, rape, physical violence, psychological abuse, and coercive control. Some women are more vulnerable to gender-based discrimination because of their race, ethnicity, class, sexuality, or other identity.[326] For example, Black women in the United States face discrimination on the basis of both their being Black and being women. Female migrant workers in the Arabian peninsula face discrimination on account of their gender, nationality, and economic vulnerability. Gender-based discrimination is prevalent in all societies, and many women who serve extreme sentences experience different forms of abuse prior to their incarceration. Gender-based violence can be perpetuated either by a stranger or by someone known to the woman. International human rights law recognizes that gender-based violence within a family, including between spouses, remains a violation of women’s human rights.[327] International human rights law obliges states to act in the face of such human rights violations. To uphold women’s human rights, states must:
- Refrain from engaging in gender-based discrimination.
- Act to prevent all forms of gender-based discrimination by private and state actors, whether direct or indirect.
- Investigate forms of discrimination where they occur.
- Provide redress for women who experience forms of gender-based discrimination.[328]
Under the due diligence framework, states should not merely abstain from violating women’s right to be free from gender-based discrimination, but must also adopt affirmative measures to protect women’s rights.[329] Such measures can include:
- Passing protective legislation.
- Training law enforcement on responding to violence against women.
- Establishing resources for women who have experienced gender-based abuse, such as sexual violence shelters.[330]
These requirements arise when a state knows or should know that a woman is at risk of gender-based violence. For example, a woman may contact state or local authorities about physical abuse, she may seek medical treatment because of an injury inflicted by her spouse,[331] or a girl may speak to her schoolteachers about an assault. In all of these cases, the state has a due diligence obligation to act because state actors know that a woman is at risk of further harm. Importantly, states have a heightened due diligence obligation with respect to girls in their jurisdiction. Many human rights instruments require states to provide girls—defined as women under the age of 18[332]—with special protection, in recognition of their particularly vulnerable status.[333] Accordingly, child marriage is a form of gender-based discrimination under international human rights law.[334] All women have the right to be free from child marriage, but child and early marriage remains very common among women facing extreme sentences. If your client was married before she reached the age of 18, the state has failed to take effective measures to protect her human rights. In essence, when a state knows of gender-based discrimination and fails to take adequate action, the state has failed to discharge its due diligence obligation. A state’s failure to act with due diligence not only violates numerous human rights treaties, but it denies women their human rights.
| Dos: |
| § Investigate state actors’ knowledge of any forms of gender-based discrimination that your client has endured. This can involve retrieving school, medical, law enforcement, and social worker records to understand the extent of state knowledge. § Adopt an intersectional approach. Consider how your client’s race, ethnicity, social class, sexual orientation, and other identities affect the discrimination she has faced. § Consider your client’s particular vulnerabilities, such as age, and how they heighten the state’s obligations to her. |
Why does the due diligence framework matter?
The due diligence framework is helpful for capital defenders in two ways: (i) it shifts the burden to the state to defend its failure to protect your client’s human rights, and (ii) it creates space for you to frame your client’s narrative within a larger context of gender-based discrimination and violence, as opposed to focusing exclusively on her individual culpability. First, the due diligence framework concerns itself with state action. The question at the heart of a due diligence analysis asks: how did the state fail my client? In uncovering instances in which state actors knew or should have known about your client’s gender-based discrimination yet failed to respond, your analysis highlights state failures. This moves the burden onto the state to respond to its failures and positions your client as a victim of human rights abuses. Such an analysis does not seek to present excuses for your client’s offense, but rather to contextualize her actions and to hold the state accountable for its role. Critically, a due diligence analysis draws a connecting line between the state’s failure to protect your client and her offense. The circumstances of women’s lives before their convictions and incarceration influence their life trajectories, and often place them on a path toward criminal behavior. Consider the case of Erica Sheppard in the United States: Erica’s childhood and adolescence were characterized by her mother’s whippings, her boyfriend’s beatings, and strangers’ sexual assaults. This violence—known to yet ignored by the police and social workers—led Erica to spend her lifetime seeking shelter from harm, ultimately driving her into the path of a man who coerced her into criminal activity. Had Erica received support, stability, and safety from the various state actors whose job it was to protect her, her life—and the life of the woman in whose death she is implicated—may have looked very different. Second, the due diligence framework allows you to frame your client’s narrative beyond her position as a defendant. It allows you to humanize her client by presenting her as a victim, rather than a perpetrator. A due diligence framework will also help you, as the advocate, determine which questions you need to ask your client about her life history. Even at trial, where you may or may not make a formal argument that the state violated its due diligence obligations, you can increase judges’ and jurors’ empathy for your client by explaining how she was harmed by either (1) the absence of systems to protect her from violence; or (2) the failure of systems (and individual actors) to carry out their obligations to protect her, take action against those who harmed her, and provide redress. By doing so, you establish a degree of collective blame for the circumstances that led to her crime, and help re-direct the anger of judicial decision-makers away from your client.
Due Diligence in Action: The Case of Jenesia Philemon
Jenesia Philemon was only sixteen years old when she married a man who repeatedly beat her, stabbed her, and sexually humiliated her. His actions caused Jenesia to seek hospital care three times. Jenesia sought support from her village authorities and hospital staff, yet no one took any action to protect her. Nor did the state of Tanzania provide Jenesia with recourse to domestic violence shelters or mental health services, as required under international law. Jenesia’s living conditions led her to develop Major Depressive Disorder. Jenesia received no treatment at all for her mental illness, and no support in escaping the conditions that continually triggered the disorder. Jenesia was sentenced to death for setting a fire that led to the death of her co-wife. After the appellate courts upheld her sentence, Jenesia’s legal team petitioned the African Court on Human and Peoples’ Rights, invoking the due diligence framework described in this chapter to explain how the state failed in its obligations to protect her from gender-based violence. They also argued that because Tanzania retains the mandatory death penalty for murder, Tanzanian domestic courts were unable to take Jenesia’s experiences of gender-based violence into account in determining the appropriate sentence for her actions. This also violated Jenesia’s rights under international human rights law. Jenesia’s lawyers have demanded not only a new trial but reparations from the state for its violations of Jenesia’s human rights.
Human Rights and Dismantling Gender-Based Stereotypes
Gendered stereotyping is another form of gender-based discrimination common to the cases of women facing extreme sentences. A stereotype is a generalized preconception of how a certain social group should behave[335] (for example, that women should be chaste, or that women should be natural caregivers). The Committee on the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) has repeatedly emphasized the harm of gender-based stereotypes as a form of discrimination against women.[336] State actors, from state investigators to judges, rely on prevalent stereotypes about women to secure their death sentences by playing on the judge and jury’s expectations of how women should appear and behave. In one East Timorese case, the judge considered that a woman was guilty of murdering her husband in part because she did not protect him “as a wife . . . must [do].”[337] This defendant’s conviction thus rested on her transgression of stereotypical notions about women’s roles in marriage. In a case from the United States, prosecutors relied on stereotypical norms about women’s chastity to secure the defendant’s conviction. Here, the state presented days of testimony about the defendant’s extramarital affairs and her “provocative” clothing, asking the jury to decide whether a good and innocent woman would engage in such behavior.[338] The harmful effects of gender stereotypes are amplified when women also face discrimination based on race, nationality, disability, or gender identity. Where state actors use stereotypes about how women should behave, feel, and appear, the state’s case rests in part on impermissible gender discrimination. The state’s actions, therefore, constitute a violation of the defendant’s human rights.
| Dos: |
| § Consider objecting whenever the prosecution uses certain gendered stereotypes to attack your client’s character. Does the state’s argument encourage the decisionmaker to condemn your client based on her failure to comply with traditional stereotypes about women? § Be conscious of the stereotypes you may rely on—even inadvertently—in your client’s defense. Are you opening your client up to gender-based stereotyping? § For example, you may want to raise your client’s positive connections with her children in mitigation of her sentence. Try to anticipate how this may lead the state, the judge, and/or the jury to rely on stereotypical expectations about women as mothers, and be aware that it could open up your client to damaging testimony about how she failed to meet gendered expectations about her role as mother. |
Chapter 7: Working With the Media
“America is addicted to salacious stories and this has fed the commodification of incarceration.” —Kwaneta Harris, currently incarcerated. Media coverage of your client’s case can be invaluable. News and social media outlets serve as a primary source of information for adults all over the world, putting journalists in a unique position to frame the public perception of your client. The power that journalists hold to shape discussions about your client can be helpful but can equally be ruinous. When women stand accused of violent crimes, the media often demonizes them in a uniquely gendered way. Women who kill their husbands may be called “Black Widows.” Others may be called “witches” or “killer moms.” It is difficult to shift public perception of your client once she is demonized in the press, and these catchy, highly damaging monikers can haunt your client throughout her trial and appeals. It is therefore vital that you consider how you can control the public narrative without running afoul of your ethical duties as counsel. This chapter will help you to prepare for media engagement.
Media Coverage of Women Defendants
Studies on media coverage of women defendants indicate that stories about women who kill are of great public interest. This is in large part because women who engage in violent acts behave contrary to stereotypical expectations. Prevalent societal norms in cultures across the world dictate that violence is incompatible with femininity and womanhood.[339] Women are expected to be nurturing, pious, good mothers, and cooperative wives.[340] A woman who kills transgresses these gendered expectations because she challenges assumptions about her capacity to nurture others.[341] There is a substantial public appetite for stories about such women because their actions represent the ultimate transgression of gender norms. Many journalists feed that appetite in their coverage of women who are charged with violent crimes. Above all else, women defendants are penalized in the press for being “bad women.” A woman is “bad” when she behaves in a manner that is counter to the societal expectations of women outlined above. A woman who is promiscuous or who engages in sex work, for example, can be characterized as unfeminine and evil because her behavior does not conform to the societal expectation that women should be pious and chaste.[342] Media coverage may therefore tend to sensationalize her sexual history, which can influence how media consumers—including decisionmakers—subconsciously view her (see Chapter 5).[343] In other cases, the media may portray women as angry, vengeful, manipulative, or hypersexual. The media simplify complex narratives; for example, they may cast a woman who kills her partner as a “jealous wife” without explaining the long history of domestic violence that predated the offense. The media also reproduce cultural tropes about women who are victims of violence. For example, media coverage of a woman defendant with a background of abuse may focus on the woman’s conduct that “invited” that abuse, much in the same way that media coverage of rape often asks what a rape victim did to provoke the rape.[344] These narratives are harmful to our clients because they minimize the impact of critical mitigating evidence.
How to Work with the Media
It is essential that you approach working with the media with care, given the importance of media coverage about your client. You must have a thorough understanding of your client’s case, including her background and mitigating factors. Develop a strong theory of the case and be prepared for media narratives to challenge this story. Having said this, there are many ways to encourage helpful reporting on your client’s case.
Prepare talking points for the media on your client’s case.
Preparing a list of talking points for media outlets is helpful for journalists and for you. Think about the most sympathetic and gripping aspects of your client’s story, and consider how her story should be told. What does the public need to understand about your client’s case? Which grave injustices should be addressed? Note that media outlets may not reproduce press releases that organizations distribute widely. Be proactive in seeking out helpful journalists and engaging with them about your client’s case. If you are in a jurisdiction where ethical rules preclude you from speaking to the media, think about whether someone else can serve as a media contact. Often, a representative of a sympathetic civil society organization may be able to educate the media about issues involving violence against women. Family members may also be excellent spokespersons for your client. In each case, you will need to evaluate the potential risks for each media contact, and provide talking points where possible. One of the most effective ways to control media coverage of your case is to provide a series of written quotes from various sources (for example, a lawyer on the defense team, a civil society representative, and an expert on one of the topics that is central to your defense). In this way, you minimize any risk that your words will be taken out of context, or that you will inadvertently say something damaging to your case.
Work with journalists to develop their reporting on gender-based violence and its link to incarceration.
You should make educating the media about the factors that contribute to women’s incarceration part of your job. The overall narrative about women and crime is harmful to women defendants and is riddled with sensationalism and inaccuracies (see Chapter 4). Use the resources in this manual and those listed below to contribute to public education through the media. Your client will benefit if the wider narrative about women defendants begins to change.
Establish strong relationships with allies.
Research media outlets and journalists who will be receptive to your client’s case. Ultimately, the coverage that will have the strongest impact will come from mainstream news sources that reach the greatest number of readers/viewers/listeners. That said, it is often difficult to obtain sensitive, nuanced coverage from these outlets (particularly broadcast television). Think about cultivating relationships with sympathetic journalists from smaller outlets, including online publications. Be creative in your approach to ally-building.
In all cases and no matter the journalist, be extremely cautious about giving the media access to your client.
Speaking to journalists can be detrimental to your client’s defense and to their mental health. Be aware that media may reach out to your client directly and encourage her to decline all media requests and direct them to contact you. If your client does consent to speaking with a journalist and you trust the journalist, you should insist on being present during the interview if the prison will allow it.
Chapter 8: Further Reading
This chapter brings together resources relevant to the representation of women facing extreme sentences. The resources are organized thematically, grouped by the topics covered in each chapter of this manual. This list is by no means exhaustive. We encourage you to add to it through your own research and to explore the resources in our extensive online bibliography. For access to these resources, please email [email protected].
Chapter 2: Conditions in Jails and Prisons
The list below contains core reading relevant to the treatment of women in prison and is discussed in Chapter 2.
- UN General Assembly, The Bangkok Rules, A/RES/65/229 (2011) https://www.unodc.org/documents/justice-and-prison-reform/Bangkok_Rules_ENG_22032015.pdf.
- Brenda van den Bergh et al., Women’s Health and the Prison Setting https://www.euro.who.int/__data/assets/pdf_file/0006/249207/Prisons-and-Health,-18-Womens-health-and-the-prison-setting.pdf.
- UN General Assembly, United Nations Standard Minimum Rules for the Treatment of Prisoners (Nelson Mandela Rules), A/RES/70/175 (2015) https://undocs.org/A/RES/70/175.
- National Center for Transgender Equality, LGBTQ People Behind Bars: A Guide to Understanding the Issues Facing Transgender Prisoners and Their Legal Rights https://transequality.org/sites/default/files/docs/resources/TransgenderPeopleBehindBars.pdf.
Chapter 3: Women and Mental Health
These articles, many referenced in Chapter 3, provide further information on the importance and role of mental health investigations for mitigation purposes.
- ACLU, Report: Mental Illness and the Death Penalty https://www.aclu.org/report/report-mental-illness-and-death-penalty.
- Jason Lee & Ryan Hall, The Death Penalty in America: An Evolving Standard https://www.psychiatrictimes.com/view/death-penalty-and-mental-illness-evolving-standard.
- Sandra Babcock, Capital Punishment, Mental Illness, and Intellectual Disability: The Failure to Protect Individuals with Mental Disorders Facing Execution https://www.ohchr.org/EN/newyork/Documents/Death-Penalty-and-the-Victims-WEB.PDF.
The following resources provide further information on the symptomologies of trauma and postpartum mental disorders and their impact on representation.
- Bethany L. Brand et al., Assessing Trauma-Related Dissociation in Forensic Contexts: Addressing Trauma-Related Dissociation as a Forensic Psychologist
- Deborah Epstein & Lisa A. Goodman, Discounting Women: Doubting Domestic Violence Survivors’ Credibility and Dismissing Their Experiences https://scholarship.law.georgetown.edu/facpub/2037/.
- Kathleen Wayland, The Importance of Recognizing Trauma Throughout Capital Mitigation Investigations and Presentation https://scholarlycommons.law.hofstra.edu/hlr/vol36/iss3/11/.
- Christina Perez-Tineo, Criminal Prosecution and the Postpartum Period: A Call for More Effective Application for the Insanity Defense https://www.luc.edu/media/lucedu/law/students/publications/ahl/pdfs/Spring%202019%20Advance%20Directive.pdf.
- Meryl Schulman & Alexandra Maul, Screening for Adverse Childhood Experiences and Trauma https://www.chcs.org/media/TA-Tool-Screening-for-ACEs-and-Trauma_020619.pdf.
Chapter 4: Gender-Based Violence
The resources listed below, referenced throughout Chapter 4, each contain further tips to help you prepare for your interviews. Use these resources in tandem with the Interviewing Protocol, contained in the appendices at the end of this manual.
- NIWAP, Trauma Informed Structured Interview Questionnaires for Immigration Cases http://niwaplibrary.wcl.american.edu/wp-content/uploads/TRAUM-Tool-InterviewQuestionsSIQI-7.12.18-FINAL.pdf. This questionnaire provides specific questions regarding a client’s relationship with the person that has abused them, instances of extreme cruelty and battery, various types of harm (including physical, physiological, and emotional harm), danger assessments, psychological maltreatment, IPV coercion, involvement of third parties, and trauma-related distress.
- WITNESS, Conducting Safe, Effective and Ethical Interviews With Survivors of Sexual and Gender-Based Violence https://s3-us-west-2.amazonaws.com/librarywebfiles/Training+Materials/Training+PDFs/Guide+to+Interviewing+Survivors+of+Gender-Based+Violence/English/Conducting-Safe-Effective-and-Ethical-Interviews-with-Survivors-of-Sexual-and-Gender-Based-Violence_v1.0.pdf.
- Asmita Ghosh, How to Sensitively Interview Survivors of Sexual Violence https://feminisminindia.com/2019/11/26/sensitively-interview-survivors-gbv/.
- SVRI, Six Golden Principles for Interviewing Women Who May Have Experienced Violence https://www.svri.org/blog/six-golden-principles-interviewing-women-who-may-have-experienced-violence.
- WITNESS, Tips: Interviewing Survivors of Gender-Based Violence https://www.witness.org/new-tipsheet-interviewing-survivors-gbv/.
- UNFPA et al., GBV Assessment & Situation Analysis Tools https://www.refworld.org/pdfid/5c3465c64.pdf.
- RAINN, Tips for Interviewing Survivors, https://www.rainn.org/articles/tips-interviewing-survivors.
- Amara Legal Center, Best Practices when Interviewing a Survivor of Sexual Assault https://www.amaralegal.org/wp-content/uploads/2016/06/Interview-Guide-for-Survvivors-of-Sexual-Assault.pdf.
- WCSAP, A Guide for Developing Tools to Assess for Sexual Assault Within the Context of Domestic Violence https://www.wcsap.org/advocacy/focus-areas/ipsv/screening-questions.
- Legal Services of Northern Virginia, Interviewing and Client Counseling for Survivor/Victims of Domestic Violence https://www.lsnv.org/wp-content/uploads/2016/05/03a_Interviewing-techniques.pdf.
Chapter 5: Treatment of Women in the Criminal Legal System
We list here resources relevant to police interactions with women accused of serious crimes.
- International Association of Chiefs of Police, Successful Trauma Informed Victim Interviewing https://www.theiacp.org/sites/default/files/2020-06/Final%20Design%20Successful%20Trauma%20Informed%20Victim%20Interviewing.pdf. This resource provides trauma-informed alternatives to common questions law enforcement may ask to collect evidence. If the police fail to follow this protocol, you can use this to cross-examine them and expose their failure to follow best practices.
Chapter 6: International Human Rights Law
Below is a selection of core human rights documents relevant to the representation of women facing extreme sentences. They are organized by geographic region. For helpful information on using these legal instruments in capital defense work, see Chapter 10 of the Cornell Center on the Death Penalty Worldwide’s best practices manual for representing individuals facing death sentences, available online at: https://deathpenaltyworldwide.org/publication/representing-individuals-facing-the-death-penalty-a-best-practices-manual/.
UN Treaties and Commentary:
- International Convention on Civil and Political Rights (ICCPR) https://www.ohchr.org/en/professionalinterest/pages/ccpr.aspx.
- General comment No. 36 (2018) on the Right to Life, U.N. Doc CCPR/C/GC/36. https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/TBSearch.aspx?Lang=en&TreatyID=8&DocTypeID=11.
- Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) https://www.ohchr.org/EN/ProfessionalInterest/Pages/CEDAW.aspx.
- General Recommendation No. 35 (2017) on Gender-Based Violence Against Women, U.N. Doc CEDAW/C/GC/35. http://tbinternet.ohchr.org/_layouts/treatybodyexternal/Download.aspx?symbolno=CEDAW/C/GC/35&Lang=en.
- General Recommendation No. 33 (2015) on Women’s Access to Justice, U.N. Doc CEDAW/C/GC/33. http://tbinternet.ohchr.org/_layouts/treatybodyexternal/Download.aspx?symbolno=CEDAW/C/GC/33&Lang=en.
- Convention on the Elimination of Racial Discrimination (CERD) https://www.ohchr.org/EN/ProfessionalInterest/Pages/CERD.aspx.
- Convention on the Rights of Persons with Disabilities (CRPD) https://www.ohchr.org/EN/HRBodies/CRPD/Pages/ConventionRightsPersonsWithDisabilities.aspx.
- Convention on the Rights of the Child (CRC) https://www.ohchr.org/EN/ProfessionalInterest/Pages/CRC.aspx.
- North, Central, and South America: American Declaration on the Rights and Duties of Man https://www.oas.org/dil/access_to_information_human_right_American_Declaration_of_the_Rights_and_Duties_of_Man.pdf.
- Inter-American Convention on the Prevention, Punishment and Eradication of Violence Against Women (Belem do Para Convention) https://www.oas.org/juridico/english/treaties/a-61.html.
- Inter-Am. Comm’n H.R., Violence and Discrimination Against Women and Girls: Best Practices and Challenges in Latin America and the Caribbean, OEA/L/V/II., Doc. 233 (2019) http://www.oas.org/en/iachr/reports/pdfs/ViolenceWomenGirls.pdf.
- Jessica Lenahan (Gonzales) et al. v. United States, Case 12,626, Inter-Am. Comm’n H.R., Report No. 80/11, (2011) https://www.oas.org/en/iachr/decisions/2011/USPU12626EN.DOC.
- Case of González et al. (“Cotton Field”) v. Mexico, Preliminary Objections, Merits, Reparations, and Costs, Judgment, Inter-Am. Ct. H.R. (2009) https://www.corteidh.or.cr/docs/casos/articulos/seriec_205_ing.pdf.
Africa
- African Charter on Human and Peoples’ Rights https://www.achpr.org/legalinstruments/detail?id=49.
- Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa (Maputo Protocol) https://au.int/en/treaties/protocol-african-charter-human-and-peoples-rights-rights-women-africa.
- African Charter on the Rights and Welfare of the Child https://www.achpr.org/public/Document/file/English/achpr_instr_charterchild_eng.pdf.
Europe
- European Convention on Human Rights https://www.echr.coe.int/documents/convention_eng.pdf.
- Council of Europe Convention on Preventing and Combating Violence Against Women and Domestic Violence (Istanbul Convention) https://www.coe.int/en/web/istanbul-convention/text-of-the-convention.
- Opuz Turkey, Eur. Ct. H.R., App. No. 33401/02, (2009) https://hudoc.echr.coe.int/eng#{%22dmdocnumber%22:[%22851046%22],%22itemid%22:[%22001-92945%22]}.
Middle East
- Arab Charter on Human Rights https://www.refworld.org/docid/3ae6b38540.html.
Chapter 7: Working with the Media
There are many resources available for journalists who report on gender-based violence. Many of these can be useful tools for your engagement with the media and can prove a helpful source of information for you as you think about how to frame the narrative around your client’s case. Some of these resources are listed below.
- UNESCO, Reporting on Violence Against Women and Girls: A Handbook for Journalists / Informer sur les violencesà l’égard des filles et des femmes (UN) https://www.un.org/sexualviolenceinconflict/wp-content/uploads/2020/01/report/reporting-on-violence-against-women-and-girls-a-handbook-for-journalists/371524eng.pdf (EN) https://www.un.org/sexualviolenceinconflict/wp-content/uploads/2020/01/report/informer-sur-les-violences-a-legard-des-filles-et-des-femmes-manuel-pour-les-journalistes/371521fre.pdf (FR)
- Sonke Gender Justice, Reporting on Gender-Based Violence: A Guide for Journalists and Editors (South Africa) https://www.saferspaces.org.za/uploads/files/Reporting-on-GBV.pdf.
- Journalists against Violence Against Women, Guidelines on Media Reporting on Violence Against Women (Serbia) https://www1.undp.org/content/dam/serbia/Publications%20and%20reports/Novinarke_protiv_nasilja_EN.pdf.
- National Sexual Violence Resource Center, Reporting on Sexual Violence(USA) https://www.nsvrc.org/sexual-violence-reporting-tools.
- Centers for Disease Control and Prevention, Reporting on Sexual Violence(USA) https://vetoviolence.cdc.gov/sites/all/themes/veto_bootstrap/assets/sv-landing/SV-MediaGuide-508c.pdf.
- Minnesota Coalition Against Sexual Violence, Reporting on Sexual Violence: A Guide for Journalists (USA) http://www.ndhealth.gov/injury/nd_prevention_tool_kit/docs/2013mediamanual.pdf.
- Angles, For Journalists (UK) https://www.angles.org.uk/for-journalists/.
- Institut national de santé public, Traiter des agressions sexuelles dans les médias (Canada) https://www.inspq.qc.ca/agression-sexuelle/medias/traiter-des-agressions-sexuelles-dans-les-medias.
Gender-Sensitive Client Interview Form
This interview protocol is not intended to provide a comprehensive list of questions that lawyers should ask their clients. Rather, it focuses on some of the most important and sensitive areas of questioning for women, including trans and queer women charged with or convicted of serious crimes. We recommend that you use this guide to formulate your own questions, based on the needs of your clients and cases. Keep the following tips in mind as you plan for your interview. § Take your time in asking your client the questions below and completing this questionnaire. § Explain to your client that you are there to help them and that you will not publicly disclose any information that they wish to keep private. § Provide context for how the questions, and the answers will help you better serve them. § If/when your client answers your questions, give them ample time to respond. § In case you have the chance to conduct multiple interviews, you may want to ask more sensitive questions at later meetings once you have created a relationship with your client. This is particularly true for the questions regarding sexual violence. § In case you are short on time, we encourage you to prioritize the questions in bold, but also use your own discretion in deciding which questions are more relevant and helpful to your client’s case.
Table of Contents
DEVELOPMENTAL AND SOCIAL HISTORY 77
Physical, Verbal, And Psychological Abuse 85
POSTCONVICTION, APPEAL, AND CLEMENCY 91
BREAKING THE ICE
| Be aware of varying cultural contexts. Certain topics may not be appropriate to ask about in different parts of the world. |
| § What was your favorite thing to do before you were arrested? |
| § Can you think of a particular moment in your life when you were really happy? |
| § What was your favorite story as a child? |
| § Did you ever have any pet animals? |
| § What helps you pass the time in detention? |
BASIC DATA
| Name: | |
| Date of birth: | |
| Age: | |
| Gender: | |
| Ethnicity: | |
| Native language(s): | |
| Note all languages spoken and ask client which language they are most comfortable speaking. | |
PRISON RELATED QUESTIONS
| § Tell me about what life in prison is like for you. |
| § What is your daily schedule like in prison? |
| § What do you eat in an average day? |
| § Do you have any access to supplemental food from family or friends? |
| § Do you think you eat more or less than when you were not in prison? |
| § What is the quality of the food? |
| § Are alternative meals offered for health reasons (e.g., diabetes)? For religious reasons? |
| § What recreational activities are available to you in prison (e.g., games, prayer, church, read, crafts, exercise)? |
| § What, if any, educational and work programs do you have access to? § What, if any, religious programs are you able to participate in? § What, if any, work programs/positions are offered? Who is eligible to participate in those activities? § Please describe your cell. § How many women are in the cell with you? § During what hours are you locked inside your cell? § Do you spend time outside your cell? For what purpose? At what times? Alone, or with others? With who? How is this time supervised by staff? What activities are available during outside time? Please explain any other details regarding the time spent outside of your cell. § Do you socialize with other prisoners? When? In what context? Is this time supervised? Do you have a particular friend or group of friends in prison? Who? § How much time do you spend alone? What do you do when you are alone? § How do you get along with the women who share your cell? Please describe your relationship. § Have you taken any leadership role(s) within the prison community? If so, please describe that role(s). § How did you come into that role? Who do you work with in that role? What are your goals in that role? What is your relationship with staff in that role? Please describe your accomplishments. § Have the prison officials or prison chaplain recognized you for good behavior? Please describe all honors, certificates, promotions, positive reviews, or other recognition. § Are you still in contact with your partner/spouse? (Do not ask this question if the husband is deceased.) § Are you still in contact with your children? Who? § Are you still in contact with other family members? Who? § Do you receive visits of your family in prison? Who visits and how often? What was the date of the last visit? § Does your family provide for you? What do they provide? § Do you write to your family, can you confirm your family’s receipt of letters? § Does your family write to you? |
| Do not ask the following questions if there are prison guards who can overhear your conversation! |
| § How have you been treated by prison guards? |
| § Have you ever been punished for breaking prison rules? Please describe what happened. What was the alleged violation? What punishment did you receive, and how long did it last? § Have you been discriminated against or harassed by any prison guard or prison staff member? Please describe what happened. |
| § Have you ever been assaulted in any way by a prison guard or staff member (verbally, physically, sexually)? |
| § Can you tell me what happened? Were you injured? If so, did you receive medical treatment? What were the consequences, if any, for the prison guard or staff member? |
| § What processes exist, if any, to report discrimination, harassment, or violence by prison guards? |
| § Have you ever pursued these processes? If so, what happened? What are the risks or potential consequences of filing reports against prison guards or staff (e.g., retaliation, arbitrary disciplinary infractions)? Have you experienced any negative consequences? If so, please describe. |
| § Please describe your relationship with other prisoners. |
| § Have you ever had a disagreement or fight with another prisoner? Please describe what happened. |
| § Have you ever been targeted by other prisoners? How? Please describe what happened. § Have you ever been assaulted in any way by another prisoner [verbally, physically, sexually]? Can you tell me what happened? Were you injured? If so, did you receive medical treatment? What were the consequences, if any, for the other prisoner(s)? |
| § Has prison staff ever intentionally placed you in a situation where you would be at high risk of assault from another prisoner? What happened? |
| § What process exists, if any, to seek protection if you feel at risk for violence by staff or other prisoners (change in housing, protective custody, etc.)? Have you ever sought protection from staff or other prisoners? Why? What happened? |
| § Does separate housing exist for those who seek protection from violence? Please describe that housing. How does that housing affect your ability to participate in programming, recreation, or outdoor activities? |
| § Is housing ever used as a reward or punishment? In what way? |
| Often, prisoners will be placed in restrictive housing under the guise of protective custody as an informal punishment or form of discrimination. |
| § If relevant in your jurisdiction: What are the prison policies on strip searches? When must you undergo a strip search? Do prison guards or staff ever subject you to strip searches outside of these instances? Please describe. Are strip searches ever used as punishment or retaliation? As a tool for coercion? Please describe. |
| § Have you ever been shackled since you arrived in prison? |
| § Have you had cuffs around your hands or your legs during the transfer or while you were in the prison/your cell? |
EDUCATION
| § Can you read or write? |
| Please verify by having client read something you write. Also ask them to write a sentence. |
| § Did you go to school? § At what age did you start school? § What schools did you attend? |
| § What is your favorite memory from school? Please tell me about a story from school. |
| § How old were you when you last attended school? |
| § What was the last grade that you completed? Why did you leave school? |
| If the client says she left school because her parents could not pay school fees, find out whether they paid school fees for her siblings, and if so, whether her parents prioritized education for boys. Also, be aware that clients may say they left school, because their parents could not afford the fees, but the reality may be more complex – parents in impoverished communities may only send children to school if they are high achievers and may stop paying fees for children with learning disabilities. |
| § What kind of student were you? What was your rank in your class? Out of how many students? |
| § What did you enjoy about school? |
| § What did you dislike about school? |
| § Did your teachers discipline you in school? What reason did they give for disciplining you? How did they discipline you? Did teachers discipline other students? Please explain? |
| Often, color, religion, gender, ethnicity, and sexual orientation/gender identity play a role in who was disciplined and how harshly. |
| § What subjects were you taught in school? § What were your favorite subjects? |
| § What subjects were the most difficult for you? |
| § Did you have difficulty learning to read, spell, write, or do elementary math? |
| § (If yes) What made those subjects difficult? Did you have any other difficulties in school? |
| § Did you ever need any extra help in school? (If yes) What type of help did you need? § Did you ever receive extra help? (If yes) Please describe any support you received from the school administration, teachers, fellow students, or family members. |
| § Please describe any learning difficulties you had. Did you ever fail or repeat any school years? § Did any of your brothers or sisters stay in school longer than you? § Please describe your social experience at school. |
| Obtain details for each sibling. |
WORK
| § How did you earn money before you were arrested? § Did you work outside the home? § Did you farm? § What was your first means of earning money? How old were you? § What other ways did you earn money over time? Please describe each job. § How did your employers/supervisors treat you? Co-workers? |
| § (If married): Did your partner work to earn money? What did they do? Were earnings with you? |
| § Who taught you the work you did? How did you learn the things you did? Did others help you? |
| If your client engages in sex work, consider asking the following questions to determine whether your client can work safely and autonomously. |
| § Do you receive money or other items of value for engaging in any sexual or intimate activities? What sorts of services do you provide? Where do you usually work? |
| § How old were you when you started providing sexual services? How did you get your first job? |
| § What are some reasons that you started engaging in sex work? |
| § Have you ever been harassed or arrested by police because of your work? |
| § How do you get paid? Do you work for an agency or another person? Were you always able to keep the money you made? § Who are your clients? Can you choose your clients? What is your relationship like with them? § Did a client or anyone else ever make you feel unsafe while working? What happened? § When a client requests that you do something that you are uncomfortable with doing, are you able to say no? Has anyone ever forced you to do something or threatened you? § Are condoms or other contraceptives available to you? Do you ask clients to use a condom? Do they request that you use one? § Are you able to protect your health? Have you ever gotten sick or pregnant? What happened? § Does your job provide you with any medical help or treatment? § Do your clients have to disclose any medical conditions, including HIV or other STIs? § What are the ages of the people you work with? What is your relationship like with them? § Do you ever drink alcohol or take drugs before working? If yes, what kind? Do your clients drink or take drugs? |
| Ask the following questions to help determine if your client is or has been a victim of labor trafficking. |
| § Tell me about your job(s) before your arrest. |
| § How did you find your job? Did anyone help you find this job? What did they tell you about the job? |
| § When you started work, was it different than what you were told? If so, how? |
| § Did you have to pay or provide services to get or keep your job? |
| § Is your immigration status tied to your job? |
| § If you were maltreated during your job, were you able to complain or seek help? |
| § Were you compensated for your labor? Was the compensation the amount that you were promised? |
| § What were the working conditions like? Did you feel safe working there? |
| § Who were your coworkers? What were they like? Did they enjoy working there? |
| § Were you able to take days off? |
| § If you did not feel well, could you leave for the day? |
| § Did you feel like you could quit your job at any point safely? |
| § Were you ever forced to remain in your job? Did your employer ever threaten you? Did your employer ever hold your passport or other important documents you own while you worked there? |
Family
General and Friends
| § Are you close with anyone in your birth family? § Who are you closest to in your birth family? |
| § Who do you share secrets with (e.g., sisters, mother, etc.)? § Are there people outside of your biological relatives that you consider family? Who? How did you meet them? |
When you fill the table below, make sure you ask your client to provide you with details on their relationship with each of the persons mentioned below. When asking about their health, please also ask about mental health and head injuries.
| Relationship (if any) | Yes/No (number) | Ages | Health/ Deceased? | What was your relationship like (stories, anecdotes)? | Same household as client? (y/n) |
| Co-spouse | |||||
| Children | |||||
| Children | |||||
| Children | |||||
| Children | |||||
| Children | |||||
| Mother | |||||
| Father | |||||
| Sister(s) | |||||
| Brother(s) | |||||
| Grandparents | |||||
| Others |
Relationships and Marriage
| § If you are married, at what age did you get married for the first time? |
| With all questions relating to age, if the client does not know, please ask her to remember if she was in school at the time, who was President, or other facts that will help you determine her age. |
| § How did you meet your partner/husband/wife/girlfriend/boyfriend? |
| § Why did you marry this person? Was it a marriage by arrangement or by romantic relationship? |
| § How many times have you been married? |
| If more than once, find out details regarding each relationship—age at time of marriage, how many years married, quality of relationship, etc. |
| § Have you had other romantic relationships? Sexual relationships? |
| § How would you compare your partner’s education level to yours (same, higher, lower)? Did you finish the same level at school? |
| § Does your partner make more or less money than you? |
| § Who had control over the finances in your marriage? Did you have equal control, more control, or less control than your partner? |
| § Can you describe what it was like for you to be married to your partner? |
| § Was there a time in your marriage that was particularly happy? |
| § What was the worst time that you remember in your marriage? |
| § How did the relationship evolve over time? |
| § What did you quarrel about? |
| § Did the partner expect things of you that you did not want to do? |
| § What was uncomfortable or difficult about the marriage? |
| § How many years were you married to your partner? |
| § Did you have any co-wives? |
| § Did your husband have intimate relationships with people outside of marriage? |
| § Did you ever get separated or divorced from your partner/wife/husband? |
| Repeat the above questions for each marriage, and make sure to verify whether the prisoner was in a polygamous relationship. |
| § If you have children, at what age did you first have a child? |
| § Have you experienced any miscarriages? |
| § Have any of your children died before reaching adulthood? |
| § Who looks after your children now? |
Ask your client to list the names and ages of all people living with the client at the time of the arrest, and the person’s relationship to the client (including children, spouse(s)/partner(s), roommates, other relatives, etc.).
| Name | Age | Relationship |
CHILDHOOD
| § When you think back on your childhood, do you remember it as a happy or difficult time? Or a little of both? Can you explain why? § Please describe your childhood home. § Who lived with your family when you were a child? When, and for how long? |
| For each person, ask your client to describe them both physically and in terms of their character. |
| § Who looked after you as a child? |
| § Did anyone else look after you and your siblings when you were a child? Who? § Did you ever look after a parent? Your siblings? § What were your responsibilities in the household? § What were the responsibilities of other household members? |
| § What did you eat on a typical day? § Were there ever times when you didn’t have enough to eat? Please describe that time. |
| § What is the longest period you went without food? |
| § When you were growing up, were you taller or shorter than other children your age? |
| § When you were growing up, were you thinner or fatter than other children your age? |
| § Can you remember anything unusual happening to your family? |
| If they say yes, ask follow-up questions about what was unusual and why they felt it was unusual. |
| § Please describe a typical day in your life at age [x]. |
| Ask the client to describe a typical day at different developmental stages in their life, such as early childhood, middle childhood, and adolescence. |
| § What serious problems have people in your family faced in their lives? |
| Ask them to try and think back to their grandparents. If yes, ask for details. |
| § Did your parents have multiple spouses? |
| § How did your father and mother support the family? |
| § Has it been necessary for anyone in the family to be cared for in some way? |
| Ask them to try and think back to their grandparents and to include their children if any. If yes, ask for details. |
| § Did you go to mosque or church? Did you hold any positions of leadership? What role does religion play in your life? What role does religion play in your family’s life? |
DEVELOPMENTAL AND SOCIAL HISTORY
| The client may not have personal knowledge of the following issues, but you can ask if they have heard about any difficulties in these areas. |
| § Have you ever been told that your mother had any difficulties during her pregnancy with you? Do you know whether she had enough food to eat at that time? |
| § Did your mother use alcohol/drugs or smoke cigarettes during her pregnancy with you? |
| § Did you observe her taking alcohol/drugs or smoke cigarettes while she was pregnant with any of your siblings? Please describe. |
| § Did you hear that your mother had any difficulties with your labor or birth? |
| § What are the most difficult memories of your childhood? |
| § Were you more often angry than your siblings were? |
| § What was the most frightening thing that happened to you as a child? |
Ask your client to describe any of the following developmental, behavioral, or emotional difficulties the client had as a child (relative to someone else in the client’s family that the client grew up with).
| Symptom | details |
| Headaches | |
| Late learning to walk | |
| Late learning to talk | |
| Speech problems | |
| Bedwetting | |
| Nightmares | |
| Problems paying attention/easily distracted | |
| Depressed/sad a lot | |
| Shy/Socially awkward | |
| Were your friends the same age as you, or younger/older?</strong > | |
| Easily frustrated | |
| Poor coordination/fell a lot/poor at sports | |
| Couldn’t sit still | |
| Difficulty controlling emotions | |
| Quarrels with other children |
Provide any additional childhood notes here: ……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..…………………………………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..……………………..…………………………………………..……………………..……………………..……………………..……………………..……………………..…………
MEDICAL HISTORY
| § Have you ever been to the hospital? |
| § Have you ever sought treatment for an illness (physical or mental)? |
| Try to get as many details about the treatment and then use the chart as a backup check. This might have happened more than once, and you should discuss each occasion with the client. |
| § Have you ever seen a doctor? § How do you feel about going to see the doctor? § How have you been treated by medical professionals? § Have you ever had difficulty accessing medical treatment? If yes, how so? |
| § Have you ever been to see a traditional healer? Why? Please describe your experience(s). |
| § Please list your current medications (including contraception). |
| § Please list your past medications (including contraception). § Have you ever sought and/or taken unprescribed medications? If yes, what medications? Where did you obtain those medications? What prompted you to seek those medications outside of a medical professional? |
| § How would you describe your mental and physical health before prison? |
| § Have you suffered any illnesses since in prison? |
| § Do you have any current health issues? |
| § Have you had any other health concerns? |
| § Are you getting treatment for these conditions in prison? Do you feel that it is adequate? |
| § Do you currently have access to women’s health services, e.g., do you have access to pain medication during menstruation, to menstrual hygiene products, or to medication for menopause? |
| § If you have a child/children detained with you, how would you describe their health? |
| § Do you have access to medical care for your child/children? |
| § If you have had children, how did you feel physically during your pregnancy(ies)? |
| § How did you feel psychologically during your pregnancy(ies)? |
| § Did you experience any difficulties during your pregnancy(ies)? Physical? Mental/psychological? During labor? |
| Ask the following questions to help determine if your client suffered from postpartum depression. These questions are especially important in cases where a mother killed her baby. |
| § How did you feel, both physically and psychologically after your pregnancy(ies)? |
| § Did you feel depressed in the weeks or months after your delivery? |
| § Did you have intrusive thoughts of harming yourself or your baby? |
| § Did you suffer from thoughts of suicide? |
| § Did you experience any unusual symptoms, including: o Confusion and disorientation? o Obsessive thoughts about the baby? o Hallucinations and delusions? o Unusual sleep disturbances? o Excessive energy or irritation? |
Before asking the following questions, remind your client that anything that they do not want you to disclose publicly will remain confidential and that you are asking these questions to help them with their case and that you are not judging them. For the following substances, please write the current amount and frequency of use, and past amount and frequency.
| Substance | Current use? Amount? | Previous use? Amount? |
| Alcohol | ||
| Marijuana | ||
| Other | ||
| Other |
| § Did anyone in your family drink alcohol? Did anyone use drugs? Try to think back to your grandparents. Consider your children. |
| § How often did they drink? How much did they drink at one sitting? What kind of alcohol did they drink? Did their behavior change when they drank? How so? |
| § How often did they use drugs? How would their behavior change when they used drugs? |
| Please exercise caution when asking the following questions. Only ask them if you feel the client is open to talking about this topic. If not, it might affect their willingness to answer other personal questions below. |
| § Have you ever been tested for Sexually Transmitted Infections (STI), including HIV? |
| § If yes, have you ever tested positive? |
| § If yes, which STI had you contracted? |
| § Did you have treatment for the STI? |
| § Are you still taking that treatment? |
| If the client is HIV+, ask if they are receiving antiretrovirals, whether she receives a special diet while in prison, and/or is receiving any other treatment for her illness. |
MENTAL HEALTH ASSESSMENT
This part of the interview is essential to help you develop mitigate and reduce your client’s sentence exposure. The goals are to find out whether (1) your client ever suffered from a mental impairment of any kind, such as mental illness, intellectual disability, or brain trauma; (2) whether and how the client’s mental impairment affected her functioning before arrest; (3) whether she has developed a mental disorder since she was arrested/incarcerated; and (4) whether your client’s mental disorder can be treated such that she could successfully reintegrate into the community. You should fill out this section not only by asking your client questions but also by closely observing your client’s behavior and asking for any supporting documents (e.g., previous hospital records), taking note of any indicia of mental illness, intellectual disability, or brain trauma. REMEMBER, the distinction between mental illness and intellectual disability: mental illness is a medical condition that disrupts a person’s thinking, feeling, mood, ability to relate to others and daily functioning, while intellectual disability refers to limitations in adaptive behaviors or intellectual functions that may affect social or practical skills. The age of onset for intellectual disability is generally during a person’s developmental period; though various diagnostic criteria define this period differently (e.g., AAIDD extends this age cap to 22). Ask these questions in a matter of fact, non-judgmental tone. Begin by explaining why you are asking them. For example, you can say something like the following: “We’re going to ask you some questions that are more personal. These may be difficult to answer. You don’t have to answer anything you don’t want to, and we can stop anytime. We ask these questions because we think it is important for your legal case. I will only share this information with the attorneys who will be assisting you in your legal case. Do you have any questions before we go any further?”
General Questions
| § How are you feeling? |
| § Have you ever seen a medical officer, nurse, or doctor who talked to you about mental health? |
| § Have you ever been hospitalized for mental health reasons (i.e., because you were not feeling well in the head)? When, and for how long? Did you ever receive a diagnosis? |
| § Did you ever receive any medication for a mental health issue? |
| § Did you receive a psychiatric assessment before trial? |
Ask if your client has experienced any of the following symptoms, how they experienced the symptom, and how it affected their functioning and their relationships.
| Symptom | In general | Details (story on when and why you felt that way) | Before or after the offense | Since in prison |
| Anxiety | ||||
| Panic attacks | ||||
| Tired, lethargy | ||||
| Depressed | ||||
| Confused (i.e., disoriented) | ||||
| Loss of appetite | ||||
| Auditory hallucinations, (i.e., hearing voices, hearing things that are not there) | ||||
| Visual hallucinations, (i.e., seeing things that are not there) | ||||
| Olfactory hallucinations (i.e., smelling things that are not there) | ||||
| Tactile hallucinations (i.e., feeling things that are not there, like bugs on one’s skin) | ||||
| Felt possessed by spirits | ||||
| Dizziness | ||||
| Loss of consciousness, blackouts | ||||
| Loss of memory, disorientation (i.e., not knowing where you are and what happened) | ||||
| Abnormally upbeat, jumpy, or wired | ||||
| Increased activity, energy, or agitation | ||||
| Exaggerated sense of well-being and self-confidence (euphoria) | ||||
| Decreased need for sleep | ||||
| Unusual talkativeness | ||||
| Racing thoughts | ||||
| Distractibility | ||||
| Poor decision-making | ||||
| Impulsivity/recklessness | ||||
| Pressured speech/talking very fast | ||||
| Disorganized thoughts/mental confusion | ||||
| Marked loss of interest or feeling no pleasure in activities | ||||
| Significant weight loss or weight gain | ||||
| Feelings of worthlessness | ||||
| Either insomnia or sleeping too much | ||||
| Obsessive thoughts or behavior | ||||
| Belief that your thoughts are not your own | ||||
| Belief that someone is after you | ||||
| Belief that someone is sending you special messages | ||||
| Chronic headaches | ||||
| Thoughts of suicide/killing yourself | ||||
| Nightmares, flashbacks | ||||
| Feeling like you were separated from your body, like you weren’t present | ||||
| Other symptoms |
| § If you have experienced suicidal thoughts, have you ever attempted to take your own life? |
| § How would you manage those suicidal thoughts? |
| § Did you ever feel like you did not have control over a particular situation or over your life in general? |
| § Do you remember anyone in your family ever experiencing any of the symptoms above? |
ABUSE RELATED QUESTIONS
You want to assess if and how abuse, whether physical, emotional, verbal, or sexual, has affected your client’s mental health. Trauma can affect how a person feels about themselves and how they relate to others. The majority of women in the criminal justice system have suffered physical and/or sexual violence in their lifetimes. Asking about this history is essential in all cases and particularly for women charged with killing family members. The questions in this section may elicit extremely sensitive information. Before you begin, consider whether you and your client have adequate privacy. To protect your client from retaliation, do not share the topic of the interview with others in the area; if need be, tell others you are interviewing her about “women’s health” or “women’s experiences.” For her comfort, ask your client whether she prefers to speak to someone of a different gender, if this is a possibility. Ultimately, you should prioritize your client’s safety and comfort over the investigation. Before you dive into these questions, take time to build trust with your client. Introduce your client to everyone participating in the interview. Describe the purpose and scope of the interview. Explain to your client that consent for the conversation can be withdrawn at any point; together, choose a safe word or non-verbal cue your client can use to pause the interview if she becomes uncomfortable. Your questions should be factual, specific, open-ended, and rooted in compassion. Avoid asking questions that begin with the phrases, “why did . . . or “why didn’t you . . .,” or any other questions that may blame, shame, or demonstrate skepticism. For clarity, avoid words like “rape” or “sexual abuse.” Your client may not identify her experiences of gender-based violence as such, and you may miss key information. It is extremely important to convey that you are listening to the client’s story, that you are not judging her in any way, and that you believe her. Maintain open body language and eye contact with your client. When your client speaks, silently listen. Use non-verbal clues like head-nodding to demonstrate your attention; do not interrupt your client. Take minimal notes. The question list below is a guide, not a script; try to encourage a natural conversation with your client. If you recognize any signs or symptoms of trauma at any point during the conversation, including hyperemotional behavior, flat affect, or a shut down, offer to pause the interview and continue at another time.
Physical, Verbal, And Psychological Abuse
| Violence in the Client’s Birth Family |
| § How were you disciplined as a child when you misbehaved? Did you get disciplined more or less than your brothers/sisters? Can you tell me about one time when you were punished for something you did? |
| § Did you ever feel physically threatened as a child? Tell me more. |
| § Were there any arguments/quarrels/disagreements in your family? Tell me how these would unfold. § Did you witness any fights or disputes in your community/neighborhood? |
| § Have any other women in your family been involved in fights or disputes? Did you witness these incidents? Were they injured? If so, how? |
| § Were any men in your family involved in fights? Can you describe them for me? |
| § Were you ever physically hurt by someone outside your family? What happened? Please describe your injuries? |
| § Did you ever see anyone else, outside your home, being beaten or physically hurt? |
| Intimate Partner Violence |
| Please note that each of these questions should be asked about every significant intimate relationship the client has had. |
| § Were you ever insulted, humiliated, cursed at, or yelled at by your partner? Did your partner ever call you names? What happened? How did it make you feel? |
| § Did your partner ever minimize your feelings? Call you crazy? Blame you for problems? |
| § What were the circumstances for these verbal insults? Was there anything that would trigger them? How often did they occur? Are there patterns you can identify (e.g., after the person had been drinking)? |
| § Have you ever felt scared or threatened because of something your partner said? |
| § Did your partner threaten to kill or hurt you or someone else? Threaten you with a weapon or other object? Threaten to commit suicide? Threaten to destroy your property? |
| § Were there times where you were not free to leave or enter your house/a room when you would have wanted to? |
| § Was your partner jealous of your friends or others? Did they ever accuse you of having an affair? |
| § Did your partner ever prohibit you from seeing and/or talking to your friends and/or family? |
| § Did your partner ever prohibit you from going to school or going to work? |
| § Did your partner ever control when you could eat, sleep, or engage in other personal activities? § Did your partner ever follow you or show up unannounced somewhere you said that you would be? § Did your partner ever control your access to money? Transportation? Phone? Internet? |
| § Have you ever been physically harmed by your partner? What were the circumstances? (Please ask them to describe each incident in detail. If they say that it happened too many times to count, ask them to describe the first time, the last time, and/or the time when they were hurt the worst. Try to get as much detail as possible for as many incidents as possible). |
| § How did your partner hurt you? What physical acts did they do? Did your partner ever kick you? Slap you? Hit you? Throw things at you? Pull your hair? Grab you by the throat? |
| § How frequently did your partner hurt you? Did the severity or frequency of the harm change over time? |
| § Can you describe the injuries you received? Can you point to the places where you received them? Did you ever seek medical attention? (Please obtain specific and detailed information about injuries, treatment, names of hospitals, etc.). |
| § Did you tell anyone about the incidents? If yes, who did you tell (e.g., police, doctor, teacher, family member etc.)? How did the person respond? Were they helpful? Did you ever make a formal complaint? What happened? Were there times that you were afraid to tell someone? |
| § Who in your family knew about your partner’s violence? Was anyone else present while it was happening? What did they do in those moments? |
| § Did you ever try to escape this situation or make plans to protect yourself? Please tell me about that. |
Sexual Violence
| General |
| § Can you describe your first sexual experience for me? What was it like? How did it make you feel? How old were you? (If the client does not remember how old she was, but it’s clear she was a teenager, ask her if she had begun to menstruate at the time of the experience.) Did you understand what was happening? How was this experience different from other intimate experiences you may have had? |
| § Have you ever been intimate with another person when you didn’t want to be? (for instance, a family member, a family friend, a stranger, your partner, a friend etc.) |
| § Were there other times that this happened, either with the same person or a different person? Can you tell me about those experiences? (Ask about each experience. Women who have been sexually abused are vulnerable to re-victimization, and they may have been repeatedly abused or raped by different people). |
| § Has anyone in your life ever touched you in a sexual way that has made you feel uncomfortable (for instance, a family member, a family friend, a teacher, a stranger, your partner, a police officer, an employer, etc.)? |
| § Did anyone touch you sexually when you were a child? Did anyone say sexual things to you when you were a child? What did they say? How did it make you feel? |
| § Where were you touched? How? How often did that occur? Where did it usually occur? Were there times it happened more frequently than others? Did you notice any patterns to the touching? Was anyone else there? What did you do after? How did it make you feel? |
| § Did you feel comfortable telling anyone? Who did you tell? What did they do? Were they able to help you in a meaningful way? Did you ever provide information for a formal report? |
| § Have there been any other times when you ever felt like you could not say no to an intimate encounter? Have you ever agreed to a sexual experience because of fear of consequences for refusing? |
| With your partner(s) |
| Please specify that this could be a current partner or a past partner. |
| § Did your partner ever force you to be intimate? How often does this happen, and when did it last happen? |
| § Have you ever been intimate with your partner because you felt like you could not say no? What did you feel in these moments? What would happen if you said no? |
| § Have you ever been intimate with your partner because they threatened you? How did your partner threaten you? |
| § Has your partner ever forced you to have a sexual experience by using a weapon, or by physically hurting you? |
| § Have you ever had sex with your partner because you wanted to protect other members of your family from being physically or psychologically abused by your partner? |
| § If the client answers “yes” to any of these questions: Were you able to tell anyone about what happened? If yes, who did you tell (e.g., police, doctor, teacher, family member, etc.)? What did they do? Were they able to help you in a meaningful way? Did you ever provide information for a formal report (e.g., to police, a medical provider, traditional leader, or schoolteacher)? |
| § Did your partner ever do or say things to you during sex or intimate moments that made you feel shame, degradation, or embarrassment? Can you tell me about these experiences? |
| § Did your partner ever force or pressure you into doing things that you weren’t comfortable with? What were they? |
| § Did your partner ever threaten to reveal information about your sexual experiences to others? |
| § Are there times when sex between you or your partner was unpleasant? Why? |
| § Did you ever receive any unwanted physical pain, cuts, bruises, scars, or lasting physical injuries? |
| § Do you and your partner ever have disagreements about sex: for example, when and how often to have sex? How do you resolve those disagreements? |
| § Did your partner ever refuse to wear a condom or take other protective measures that you wanted? |
| § Do you think you and your partner enjoyed your sexual relationship equally? |
| § Has your partner ever forced you to have a sexual experience by kidnapping you, or by breaking into your home or someone else’s home? |
| § Has your partner ever had sex with you when you were intoxicated or physically/mentally unable to say yes or agree to the activity? |
| § Did you ever do things to avoid sexual activity with your partner? Avoid certain parts of the house? |
Harm Assessment
| § How have these any of these experiences changed your mental and physical energy? |
| § Do you still have any physical pain? What is the intensity and duration like? Are you taking any medication? |
| § Do you experience any sleeping problems, depression, anxiety, humiliation, shame, or other negative feelings because of these instances? How do you cope with these emotions? Are you still able to engage in activities that bring you peace and joy? Have you considered or sought counseling? |
| § When you remember these instances, do you experience any of the following: |
| o Stress or intense emotions? |
| o Physical reactions like pounding heartbeat, sweating, breathing difficulties, or trembling? |
| o Numbness? |
| o An inability to think, concentrate, or process information? |
| o Feeling very alert and aware of your surroundings? |
| § Do you avoid thinking about these experiences? Do you have difficulty remembering these events? Do you ever have nightmares about them? |
| § How has your behavior and mood changed generally? Do you have angry outbursts? Are you able to work or be productive? Has it changed the way you relate to others? Are you more fearful or mistrustful of others? What about others who experienced or witnessed these incidents (children, siblings, etc.)? |
| § What are your fears for the future? |
| § What are your hopes for the future? |
| § Are there any other experiences or feelings you would like to share? |
| § How are you feeling right now? |
| § Would you be interested in information about resources for psychological, emotional, or physical support? Any other resources that could help with healing and recovery? |
When you are done asking questions to the client about violence, abuse and mental health, we encourage you to take some time to thank them for sharing this information with you and to recognize the difficulty of the conversation. Spend time attending to any feelings that may have arisen for the client during this conversation. Ask the client if they would like to share any other experiences with you. Remind them that everything that they do not want you to disclose publicly will remain confidential. Most importantly, because this conversation may have brought back some very painful memories, reassure them that they are not responsible for what happened to them, that they are not alone and that you will do your best to help them with their case. If your client is still distressed, consider doing breathing exercises or meditations to ease them. Offer information on relevant services to support your client. Let your client know what the next steps in the case will be and remind them that the information they provided will be helpful moving forward.
PHYSICAL HEALTH ASSESSMENT
| § How is your appetite? |
| § Have you experienced any recent gain or loss without change in diet? |
| § How is your sleep? |
| § How many hours do you sleep? |
| § Do you feel tired? |
| § Do you have energy to do the things you want to do? |
| § How is your ability to focus & concentrate? Do you find it hard to concentrate on one task for a long time? |
| § How is your memory? Do you sometimes find it hard to remember something that you normally know? |
| § Have you ever lost consciousness? |
| § Have you ever lost your sense of time? (For example, did anyone ever tell you that you were behaving unusually, and you had no memory of it? Details: what age, how long, how often, were there any witnesses). |
| § Do you menstruate regularly? |
| § Have you noticed any changes in your menstruation (e.g., length, irregularities, etc.)? |
| Ask in general, at the time of the offense, and since in prison. |
| § Can you manage your own self-care (i.e., bathing, dressing, washing your own clothes, etc.)? If not, who helps you? |
| § Have you noticed any changes in your routines and preferences for self-care? |
ARREST AND OFFENSE
| Ask the following questions if the client is charged along with a co-defendant. |
| § What was your relationship to the person (or people) you were arrested with? |
| § Did anyone threaten or pressure you to commit the offense that you are charged with? What did they say or do to threaten you? |
| § Did anyone make a promise to you in exchange for your agreement to do something? |
| Ask the following questions if the client had interactions with police. Ask them for each arrest of interaction. |
| § How did the police treat you when you were arrested? Describe what happened during the arrest. |
| § (If client has children) Who was taking care of your children when you were arrested? |
| § Were you shackled at the time of arrest? Where did the police take you? Can you describe what it looked like in the room? Were you placed in a cell? Were other people in the cell with you? What was the age range of individuals in that placement? What was the range of offenses for which individuals were placed in that facility? |
| § Describe your interactions with staff at that facility. Describe your interaction with other incarcerated persons at that facility. How long were you in that location? |
| § Have you ever been arrested before this offense? |
| § Describe any other interactions with police, including those that did not result in arrest. |
| § Did you make a statement to the police? |
| § Describe the environment when you were questioned. Please describe your interrogation. |
| § Were you handcuffed or shackled? |
| § What was the gender of each police officer who interrogated you? How many police officers were in the room with you? |
| § Did they threaten you in any way? Did the police promise you anything if you would confess? Please describe. |
| § Did the police harm you physically in any way? |
| § Did the police make any insulting or sexual comments to you? Please tell me more. |
| § Did the police ever threaten your children or family? |
| § Had you eaten? Had you slept? Did you have anything to drink? |
| § How long did they ask you questions? |
| § How long were you in custody before you gave them a statement? |
| § How were you feeling physically at the time you gave your statement? |
| § Did anyone tell you that you could ask for a lawyer or remain silent? |
POSTCONVICTION, APPEAL, AND CLEMENCY
Lawyer
| § Tell me about your lawyer. What was your relationship like? |
| § What type of lawyer did you have (Legal Aid, private, etc.)? |
| § What was your lawyer’s name? |
| § How many months were you in prison before you saw a lawyer for the first time? |
| § Did your lawyer visit you in prison before trial? How many times? For how long? |
| Note approximate dates if the client remembers. |
| § Did you have a conversation with your lawyer on the day of your trial? |
| § How long did your lawyer speak to you? |
| § Did your lawyer ever ask you about your relationship with your spouse (if married)? § Did your lawyer ever ask you the questions I’ve asked you about your prior experiences of violence? |
| § Which topics/what information did you discuss with your lawyer? § Did your lawyer ever speak to your family or to other individuals from your life? |
| Try to understand if mental health, violence, or trauma were ever previously discussed. |
| § (If you had a co-defendant) Were you represented by the same lawyer as your co-defendant? |
Trial
| § How did it feel for you to be on trial? |
| § What did you understand? |
| § What was/were the most difficult part/s? |
| § What felt confusing? |
| § Did you testify about the violence you had experienced in your life? |
| § If relevant: Did you or anyone else testify about your husband’s abuse? What kinds of questions were you asked, and what did you say? |
| § What arguments were made by your lawyer for a sentence other than death? |
| § (If you had a co-defendant) What was your relationship with the co-defendant? Did you interact with the co-defendant during the trial, and if so, what did you discuss? |
| § Did you need an interpreter? |
| § If so, did the court provide one and were they always there? Were they helpful? |
| § Did someone explain to you what had happened during the trial and what the outcome was? |
Endnotes
[1] See World Health Organization
Definition of Gender; American Psychological Association, Guidelines for
Psychological Practice with Transgender and Gender Nonconforming People Vol. 70,
No. 9, 832-864. (2015) available at
https://www.apa.org/practice/guidelines/transgender.pdf; American
Psychological Association, Guidelines for Psychological Practice with Lesbian,
Gay, and Bisexual Clients. (2012) available at https://www.apa.org/pi/lgbt/resources/guidelines.
[2] American Psychological Association,
Guidelines for Psychological Practice with Transgender and Gender Nonconforming
People Vol. 70, No. 9, 832-864. (2015) available at
https://www.apa.org/practice/guidelines/transgender.pdf; American
Psychological Association, Guidelines for Psychological Practice with Lesbian,
Gay, and Bisexual Clients. (2012) available at https://www.apa.org/pi/lgbt/resources/guidelines.
[3] See also American
Psychological Association, Guidelines for Psychological Practice with
Transgender and Gender Nonconforming People Vol. 70, No. 9, 832-864. (2015),
available at
https://www.apa.org/practice/guidelines/transgender.pdf; American
Psychological Association, Guidelines for Psychological Practice with Lesbian,
Gay, and Bisexual Clients. (2012) available at https://www.apa.org/pi/lgbt/resources/guidelines.
[4] See also American
Psychological Association, Guidelines for Psychological Practice with
Transgender and Gender Nonconforming People Vol. 70, No. 9, 832-864. (2015)
available at
https://www.apa.org/practice/guidelines/transgender.pdf; American
Psychological Association, Guidelines for Psychological Practice with Lesbian,
Gay, and Bisexual Clients. (2012) available at https://www.apa.org/pi/lgbt/resources/guidelines.
[5] The DSM-5 refers to the Fifth Edition
of the Diagnostic and Statistical Manual of Mental Disorders, the standard
classification of psychiatric diagnoses used by mental health professionals in
the United States.
[6] See, e.g., United Nations
General Assembly Resolution 67/187, United Nations Principles and Guidelines on
Access to Legal Aid in Criminal Justice Systems (stating that “special measures
should be taken to ensure meaningful access to legal aid for women, children and
groups with special needs” and that “such measures should address the special
needs of those groups, including gender-sensitive and age-appropriate
measures”); Id. (“States should take applicable and appropriate
measures to ensure the right of women to access legal aid, including: (a)
Introducing an active policy of incorporating a gender perspective into all
policies, laws, procedures, programmes and practices relating to legal aid to
ensure gender equality and equal and fair access to justice; (b) Taking active
steps to ensure that, where possible, female lawyers are available to represent
female defendants, accused and victims”); Id. (“States should ensure
that mechanisms to track, monitor and evaluate legal aid are established and
should continually strive to improve the provision of legal aid,” which could
include “provid[ing] cross-cultural, culturally appropriate, gender-sensitive
and age-appropriate training to legal aid providers”); United Nations Convention
on the Elimination of all Forms of Discrimination against Women (CEDAW)
Committee’s General Recommendation 19 (1992) (providing that “gender-sensitive
training of judicial officers is essential for the effective implementation of
CEDAW”); Updated Model Strategies and Practical Measures on the Elimination
of Violence against Women in the Field of Crime Prevention and Criminal Justice
(ECOSOC resolution 2010/15, annex, adopted on 22 July 2010) (urging member
states to “provide for or to encourage mandatory
cross-cultural, gender and child-sensitivity training
modules for police, criminal justice officials and professionals
involved in the criminal justice system on the unacceptability of all forms
of violence against women and on their harmful impact and consequences on all
those who experience such violence (para. 20-a));
United Nations Rules for the Treatment of Women Prisoners and
Non-custodial Measures for Women Offenders (the Bangkok Rules, ECOSOC
resolution 2010/16, annex, adopted on 22 July 2010) (providing that “[i]n order
for the principle of non-discrimination, embodied in the rule 6 of the Standard
Minimum Rules for the Treatment of Prisoners to be put into practice, account
shall be taken of the distinctive needs of women prisoners in the application
of the Rules” and “Efforts shall be made to review, evaluate and
make public periodically the trends, problems
and factors associated with offending behaviour in women and the effectiveness
in responding to the social reintegration needs of women
offenders, as well as their children, in order to reduce the stigmatization
and negative impact of those women’s confrontation with the criminal justice
system (Rule 69).”); United Nations Office on Drugs and Crime, Gender in the
Criminal Justice System Assessment Tool at 1 (2010),; available at
https://www.unodc.org/documents/justice-and-prison-reform/crimeprevention/E-book.
>pdf (“Identifying and understanding the realities of women and men
in the community as well as the gender biases that may promote discrimination,
limit access to justice and prevent women’s full participation in the criminal
justice system underpin any assessment of the criminal justice system”).
[7] See, e.g., Supplementary
Guidelines for the Mitigation Function of Defense Teams In Death Penalty Cases,
36 Hofstra Law Review 677, 682-683 (2008) (“The defense team must include
individuals possessing the training and ability to obtain, understand, and
analyze all documentary and anecdotal information relevant to the client’s life
history,” including “religious, gender, sexual orientation, ethnic, racial,
cultural and community influences; socio-economic, historical, and political
factors.”); id. at 683 (“Mitigation specialists must be able to
identify, locate, and interview relevant persons in a culturally competent
manner that produces confidential, relevant and reliable information.”),
available at
https://law.hofstra.edu/pdf/academics/journals/lawreview/lrv_issues_v36n03_cc1_guidelines_final.pdf
>
[8] United Nations Principles and
Guidelines on Access to Legal Aid in Criminal Justice Systems, Guideline 9(b),
(Apr. 26 2012), available at
https://archive.crin.org/en/library/legal-database/un-principles-and-guidelines-access-legal-aid-criminal-justice-systems.html
>.
[9] Black and Pink, Coming Out of Concrete
Closets: A Report on Black & Pink’s National LGBTQ Prisoner Survey (2015),
available at
https://law.hofstra.edu/pdf/academics/journals/lawreview/lrv_issues_v36n03_cc1_guidelines_final.pdf
>.
[10] Id.
[11] Much of the content of this section
was first published in the Cornell Center on the Death Penalty Worldwide’s
seminal report on women facing death sentences. See The Cornell Center
on the Death Penalty Worldwide, Judged for More Than Her Crime: A Global
Overview of Women Facing the Death Penalty (Sept. 2018), available at
https://secureservercdn.net/198.71.233.33/l8z.2c6.myftpupload.com/wp-content/uploads/2019/12/Judged-More-Than-Her-Crime.pdf?time=1629925047
>.
[12] For example, in the United States,
40% of incarcerated women identify as lesbian or bisexual. Ilan H. Meyer, et al.
Incarceration Rates and Traits of Sexual Minorities in the United States:
National Inmate Survey, 2011-2012, 107 AMERICAN JOURNAL OF PUBLIC HEALTH 2
(2017), available at
https://pubmed.ncbi.nlm.nih.gov/27997242/. This high rate of incarceration is
even greater for LGBTQ+ individuals who are low-income, immigrants,
transgender, and people of color. Although it is difficult to identify the
number of trans women globally who are incarcerated, it is clear that trans
women experience some of the highest rates of incarceration. In Australia, one
study revealed that 60% of formerly incarcerated transgender informants were
of Australian Aboriginal background. Annette Brömdal, et al.,
Whole-incarceration-setting approaches to supporting and upholding the rights
and health of incarcerated transgender people, 20 INTERNATIONAL JOURNAL OF
TRANSGENDERISM 4 (Aug. 16, 2019). In a study in the U.S., nearly 50% of black
trans women respondents had been incarcerated, about 20 times the rate of the
general population in the U.S. Sandy E. James, et al., The report of the 2015
U.S. Transgender Survey, NATIONAL CENTER FOR TRANSGENDER EQUALITY (Dec. 2016),
available at https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf
>.
[13] See Inter-American
Commission on Human Rights, Violence against LGBTI Persons, Doc. 36 (2015),
available at
https://www.oas.org/en/iachr/reports/pdfs/ViolenceLGBTIPersons.pdf
>; see also National Center for Transgender Equality, LGBTQ People
Behind Bars, 5, available at https://transequality.org/sites/default/files/docs/resources/TransgenderPeopleBehindBars.pdf
>.
[14] See Inter-American
Commission on Human Rights, Violence against LGBTI Persons, Doc. 36 (2015),
available at
https://www.oas.org/en/iachr/reports/pdfs/ViolenceLGBTIPersons.pdf
>.
[15] UN General Assembly, Resolution
adopted by the General Assembly on 21 December 2010: The Bangkok Rules,
A/RES/65/229 (Mar. 16, 2011), available at
https://www.unodc.org/documents/justice-and-prison-reform/Bangkok_Rules_ENG_22032015.pdf
>.
[16] Id. at Rules 2, 6.
[17] Id. at Rules 19–21.
[18] Id. at Rule 22. UN General Assembly,
United Nations Rules for the Protection of Juveniles Deprived of their Liberty,
Rule 67 (Dec. 14, 1990), available at
https://www.un.org/ruleoflaw/files/TH007.PDF.
[19] UN General Assembly, Resolution
adopted by the General Assembly on 21 December 2010: The Bangkok Rules,
A/RES/65/229, Rules 13, 29, 32–35 (Mar. 16, 2011), available at
https://www.unodc.org/documents/justice-and-prison-reform/Bangkok_Rules_ENG_22032015.pdf
>.
[20] Id. at Rules 29–30.
[21] Id. at Rules 5, 11.
[22] Id. at Rule 60.
[23] Id. at Rules 12, 41.
[24] Id. at Rules 4, 28, 43.
[25] Id. at Rule 56.
[26] Id. at Rules 36–39.
[27] Id. at Rule 53.
[28] Id. at Rule 54.
[29] Id. at Rules 5, 15, 22, 42.
[30] Id. at Rules 23.
[31] Id. at Rules 49–52.
[32] Id. at Rules 11.
[33] Id. at Rules 74, 76, 81.
[34] Id. at Rules 15, 16, 18–21.
[35] Id. at Rule 48.
[36] Id. at Rules 4, 58–60, 68, 70.
[37] Shamas Jalil, affiliated with
Strengthening Participatory Organization, Interview with Justice Project
Pakistan, Jul. 25, 2017, cited in Justice Project Pakistan, Research Report to
the Cornell Center on the Death Penalty Worldwide, Jul.–Aug. 2017. Anonymous
Source, Research Report to the Cornell Center on the Death Penalty Worldwide,
Jul. 19, 2017.
[38] Cassandra Abernathy, Research Report
to the Cornell Center on the Death Penalty Worldwide, May 2018; Pamela
Okoroigwe, Noel Brown, Abiodun Odusote, Interview with the Cornell Center on the
Death Penalty Worldwide, Jun. 19, 2017.
[39] For example, see Arizona
Dept. of Corrections, Death Row Information and Frequently Asked Questions,
https://corrections.az.gov/public-resources/death-row/death-row-information-and-frequently-asked-questions
>, last accessed Jun. 28, 2018.
[40] See Introductory Language.
[41] Annette Brömdal, et al.,
Whole-incarceration-setting approaches to supporting and upholding the rights
and health of incarcerated transgender people, 20 INTERNATIONAL JOURNAL OF
TRANSGENDERISM 4 (Aug. 16, 2019).
[42] In the U.S., the Prison Rape
Elimination Act (PREA) and Department of Justice guidance issued in 2016 called
for individual determinations of housing, program, and other assignments in
correctional facilities. That means an individual assessment must be made,
taking many factors into account, including the person’s own views about their
gender and safety. It also made assigning a transgender prisoner to housing,
programs, or other services based solely on their sex assigned at birth a
violation of federal law. In 2016, however, the Bureau of Prisons changed its
policy so that “biological sex” will be used as the basis for the initial
determination and transgender prisoners will be assigned to facilities
conforming to their gender identity only “in rare cases.”
[43] United Nations General Assembly,
Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, Note by
the Secretary-General, U.N. Doc. A/66/268 (5 August 2011).
[44] One study revealed that 85% of
LGBTQ+ prisoners in the U.S. have been placed in solitary confinement for their
own safety, effectively punishing LGBTQ+ prisoners for their identity rather
than identifying other alternatives to prevent abuse. Indeed, 50% of respondents
who were placed in solitary confinement were put there against their will. Due
to inappropriate placement of LGBTQ prisoners, especially transgender women,
these individuals are often forced to choose between the torture of sensory
deprivation and threat of violence from other prisoners in general population.
[45] It is important not to presume how a
client wishes to express their gender identity and to consult with clients about
how best to advocate for them. For example, some clients may not openly identify
as LGBTQ while incarcerated due to safety concerns and may not want to challenge
housing classifications or policies, while others may want to pursue other
housing options and/or challenge gender-restrictive policies.
[46] LBH Masyarakat, Research Report to
the Cornell Center on the Death Penalty Worldwide, Sep. 9, 2017.
[47] Rosemary Barberet, Women, Crime and
Criminal Justice: A Global Enquiry, ROUTLEDGE, 165 (2014).
[48] Brenda van den Bergh, et al.,
Women’s health and the prison setting, PRISONS AND HEALTH, 161, available at
https://www.euro.who.int/__data/assets/pdf_file/0006/249207/Prisons-and-Health,-18-Womens-health-and-the-prison-setting.pdf
>.
[49] Maiko Tagusari, affiliated with
Center for Prisoners’ Rights, Interview with the Cornell Center on the Death
Penalty Worldwide, Mar. 6, 2015.
[50] Danthong Breen, affiliated with
Union of Civil Liberties, Interview with the Cornell Center on the Death Penalty
Worldwide, Mar. 23, 2015; Roxanne Daniel, Prisons Neglect Pregnant Women in
Their Healthcare Policies, PRISON POLICY INITIATIVE (Dec. 5, 2019), available at
https://www.prisonpolicy.org/blog/2019/12/05/pregnancy/; Anonymous Source,
Interview with the Cornell Center on the Death Penalty Worldwide, Feb.
2016.
[51] Brenda van den Bergh, et al.,
Women’s health and the prison setting, PRISONS AND HEALTH, 160–161, available at
https://www.euro.who.int/__data/assets/pdf_file/0006/249207/Prisons-and-Health,-18-Womens-health-and-the-prison-setting.pdf
>.
[52] See Introductory Language.
[53] Gender Dysphoria is a disorder in
the Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 that refers to
the feeling of discomfort or distress that might occur in people whose gender
identity differs from their sex assigned at birth or sex-related physical
characteristics. Gender Dysphoria replaced the diagnosis of Gender Identity
Disorder in the DSM-IV and focuses more on the discomfort experienced by some
gender diverse individuals rather than a person’s gender identity in and of
itself. The International Statistical Classification of Diseases and Related
Health Problems (ICD)-11 arguably goes even farther in depathologizing
transgender and gender non-conforming identities, replacing the ICD-10 diagnoses
of “transsexualism” and “gender identity disorder of children” with “gender
incongruence of adolescence and adulthood” and “gender incongruence of
childhood.” ICD-11 characterizes “gender incongruence” as “a pronounced,
persistent incongruence between the individual’s experience of gender and the
sex assigned” during adulthood and childhood, respectively. See Rebeca
R. García & José L. Ayuso-Mateos, ICD-11 and the depathologisation of the
transgender condition, 12 REVISTA DE PSIQUIATRIA Y SALUD MENTAL 67 (2019),
available at
https://www.elsevier.es/en-revista-revista-psiquiatria-salud-mental-486-articulo-icd-11-depathologisation-transgender-condition-S2173505019300214
>. The ICD-11 also moved “gender incongruence” from the chapter on “Mental
and behavioral disorders” to the new chapter on “Conditions related to sexual
health,” recognizing that individuals who are transgender and gender diverse
are not necessarily mentally ill, but have specific health needs. At the same
time, they experience barriers to accessing gender-affirming health care, and
are at higher risk of exposure to violence and other health risks, such as
sexually transmitted infections. See World Health Organization,
WHO/Europe brief—transgender health in the context of ICD-11, available at https://www.euro.who.int/en/health-topics/health-determinants/gender/gender-definitions/whoeurope-brief-transgender-health-in-the-context-of-icd-11
>.
[54] For example, in 2015, 385 prisoners
in California were receiving “cross-sex hormone therapy,” but no
gender-affirming surgery had been offered by any U.S. correctional facility
unless ordered by a court. Jae Sevelius & Valerie Jenness, Challenges and
opportunities for gender-affirming healthcare for transgender women in prison,
13 INTERNATIONAL JOURNAL OF PRISON HEALTH 1, 32–40 (Mar. 13, 2017), available at
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8263052/.
[55] Many carceral institutions argue
that they will not provide gender-affirming health care for safety reasons,
including classification and housing, and/or financial reasons. Still other
institutions that understand the implications of failing to provide medical care
for a diagnosable mental health disorder and physical medical conditions claim
that trans or non-binary prisoners are malingering.
[56] American Medical Association,
Transgender prisoners have fundamental right to appropriate care (May 17, 2019),
available at
https://www.ama-assn.org/delivering-care/population-care/transgender-prisoners-have-fundamental-right-appropriate-care
>
[57] Jae Sevelius & Valerie Jenness,
Challenges and opportunities for gender-affirming healthcare for transgender
women in prison, 13 INTERNATIONAL JOURNAL OF PRISON HEALTH 1, 32–40 (Mar. 13,
2017), available at
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8263052/.
[58] Josefina Alfonsin, et al., Trans
Women Deprived of Liberty: Invisible Stories Behind Bars, 10, available at
https://www.wola.org/wp-content/uploads/2020/04/Trans-Women-Deprived-of-Liberty.-Invisible-Stories-Behind-Bars_Final-3.pdf(quoting CELS, Informe alternativo “El cumplimiento del Estado argentino
de la Convención contra la tortura” (Mar. 23, 2017), available at http://www.cels.org.ar/web/wp-content/uploads/2017/05/Informe-alternativo-CAT-2017.pdf.).
>
[59] Jason Lydon, et al., Coming Out of
Concrete Closets: a Report on Black and Pink’s National LGBTQ Prisoner Survey, 2
BLACK & PINK, 4 (Oct. 21, 2015), available at
https://www.issuelab.org/resources/23129/23129.pdf.
[60] Many transgender and non-binary
individuals face institutional barriers to accessing gender-affirming medical
care, including transphobia among medical providers, lack of health insurance,
and prohibitive costs. These barriers may prevent a person from ever receiving
transition-related care or from obtaining such treatment legally. See,
e.g. Josefina Alfonsin, et al., Trans Women Deprived of Liberty:
Invisible Stories Behind Bars, 10, available at
https://www.wola.org/wp-content/uploads/2020/04/Trans-Women-Deprived-of-Liberty.-Invisible-Stories-Behind-Bars_Final-3.pdf(explaining that “the human rights violations experienced by trans people
include misinformation by medical personnel regarding available care options
and the rules for providing hormone treatment” and citing a survey by
Argentina’s National Institute of Statistics and Censuses revealing that 48.7%
of trans people have stopped going to the doctor due to discrimination on the
basis of gender identity).
[61] See Building a
Gender-Sensitive Team.
[62] Johnson John Mbwambo, affiliated
with the Legal and Human Rights Centre, Tanzania, Interview with the Cornell
Center on the Death Penalty Worldwide, Jun. 14, 2017.
[63] See, e.g., Mona El-Naggar,
et al., When a Search Crosses the Line, NEW YORK TIMES (Jul. 5, 2021), available
at
https://www.nytimes.com/interactive/2021/07/05/world/middleeast/egypt-sexual-assault-police.html(interviewing Egyptian women subjected to sexual harassment and violence
in police stations, prisons and hospitals).
[64] See, e.g., Health Policy
Project, Asia Pacific Transgender Network, U.N. Development Programme, Blueprint
for the Provision of Comprehensive Care for Trans People and Trans Communities
in Asia and the Pacific, 18 (2015), available at
http://www.healthpolicyproject.com/pubs/484_APTBFINAL.pdf (“The UN Special
Rapporteur on torture has raised concerns that trans people are one of the
groups at the bottom of the prison hierarchy, and that trans women detained
within the general prison population are at risk of physical and sexual
abuse.”) (quoting the Office of the High Commissioner for Human Rights
(2011)). “LGBTQ prisoners are over six times as likely to be sexually
assaulted as the general prison population, with transgender women, nonbinary
people, and other gender nonconforming prisoners at particular risk.” ACLU,
Still Worse Than Second-Class: Solitary Confinement of Women in the United
States, 10 (2019), available at https://www.aclu.org/report/worse-second-class-solitary-confinement-women-united-states
>. For example, two out of three black and Latina trans women incarcerated
in the U.S. report having been sexually assaulted while incarcerated. Center
for American Progress and Movement Advancement Project, Unjust: How the broken
criminal justice system fails LGBT people (2016), available at http://www.lgbtmap.org/file/lgbt-criminal-justice.pdf.
[65] Amnesty Intl., Stonewalled: Police
abuse and misconduct against lesbian, gay, bisexual and transgender people in
the U.S., AMR 51/122/2005 (Sept. 2005), available at
https://www.amnesty.org/en/wp-content/uploads/2021/08/amr511222005en.pdf
>.
[66] National Center for Transgender
Equality, Failing to Protect and Serve: Police Department Policies Towards
Transgender People (2019), available at
https://transequality.org/sites/default/files/docs/resources/FTPS_ES_v3.pdf
>.
[67] Neela Ghoshal, In Cameroon
Transgender Women Given Five-Years in Prison, HUMAN RIGHTS WATCH (May 12, 2021),
available at
https://www.hrw.org/news/2021/05/12/cameroon-transgender-women-given-five-years-prison
>.
[68] Blueprint for the Provision of
Comprehensive Care for Trans People and Trans Communities in Asia and the
Pacific, 18 (2015), available at
http://www.healthpolicyproject.com/pubs/484_APTBFINAL.pdf (“Trans women are
likely to be over-represented within the prison population in those countries
within the [Asia and the Pacific] region that criminalise sex work or
cross-dressing, or use public nuisance and vagrancy laws to harass trans
women,” which is linked to “grave violence against trans women detained in
male lockups or prison cells”).
[69] Jason Lydon, et al., Coming Out of
Concrete Closets: a Report on Black and Pink’s National LGBTQ Prisoner Survey, 2
BLACK & PINK, (Oct. 21, 2015), available at
https://www.issuelab.org/resources/23129/23129.pdf.
[70] Just Detention International,
Targets for Abuse: Transgender Inmates and Prisoner Rape (Mar. 2013), available
at
https://justdetention.org/wp-content/uploads/2015/10/FS-Targets-For-Abuse-Transgender-Inmates-And-Prisoner-Rape.pdf
>.
[71] See, e.g., Josefina
Alfonsin, et al., Trans Women Deprived of Liberty: Invisible Stories Behind
Bars, 10, available at
https://www.wola.org/wp-content/uploads/2020/04/Trans-Women-Deprived-of-Liberty.-Invisible-Stories-Behind-Bars_Final-3.pdf(explaining that throughout South America, LGBTQ+ prisoners face “verbal,
psychological, and physical violence, in particular sexual violence
perpetrated by prison staff or other detainees,” as well as “prolonged
solitary confinement” and “torture”); Blueprint for the Provision of
Comprehensive Care for Trans People and Trans Communities in Asia and the
Pacific, 18 (2015), available at http://www.healthpolicyproject.com/pubs/484_APTBFINAL.pdf (describing
physical and sexual violence against transgender prisoners in Asia and the
Pacific).
[72] See, e.g., Jason Lydon, et
al., Coming Out of Concrete Closets: a Report on Black and Pink’s National LGBTQ
Prisoner Survey, 2 BLACK & PINK, (Oct. 21, 2015), available at
https://www.issuelab.org/resources/23129/23129.pdf; Josefina Alfonsin, et
al., Trans Women Deprived of Liberty: Invisible Stories Behind Bars, 15,
available at https://www.wola.org/wp-content/uploads/2020/04/Trans-Women-Deprived-of-Liberty.-Invisible-Stories-Behind-Bars_Final-3.pdf(In El Salvador’s prisons, LGBTI+ people are subject to grave human
rights violations during body searches, including torture, ill-treatment,
physical aggression, and rape fostered by the security system).
[73] Blueprint for the Provision of
Comprehensive Care for Trans People and Trans Communities in Asia and the
Pacific, 18 (2015), available at
http://www.healthpolicyproject.com/pubs/484_APTBFINAL.pdf,
[74] See, e.g., Josefina
Alfonsin, et al., Trans Women Deprived of Liberty: Invisible Stories Behind
Bars, 10, available at
https://www.wola.org/wp-content/uploads/2020/04/Trans-Women-Deprived-of-Liberty.-Invisible-Stories-Behind-Bars_Final-3.pdf
>; Just Detention International, Targets for Abuse: Transgender Inmates and
Prisoner Rape (Mar. 2013), available at https://justdetention.org/wp-content/uploads/2015/10/FS-Targets-For-Abuse-Transgender-Inmates-And-Prisoner-Rape.pdf
>.
[75] Josefina Alfonsin, et al., Trans
Women Deprived of Liberty: Invisible Stories Behind Bars, 10, available at
https://www.wola.org/wp-content/uploads/2020/04/Trans-Women-Deprived-of-Liberty.-Invisible-Stories-Behind-Bars_Final-3.pdf
>.
[76] For an overview of the death penalty
and mental illness, See ACLU, Report: Mental Illness and the Death
Penalty (May 5, 2009), available at
https://www.aclu.org/report/report-mental-illness-and-death-penalty
>; Jason Lee & Ryan Hall, The Death Penalty in America: An Evolving
Standard, 34 Psychiatric Times 6 (June 21, 2017), available at https://www.psychiatrictimes.com/view/death-penalty-and-mental-illness-evolving-standard
>; Mental Health America, Position Statement 54: Death Penalty and People
with Mental Illnesses (last accessed Mar. 21, 2021), available at https://www.mhanational.org/issues/position-statement-54-death-penalty-and-people-mental-illnesses
>; Death Penalty Information Center, Mental Illness (last accessed Mar. 21,
2021), available at https://deathpenaltyinfo.org/policy-issues/mental-illness.
See also Sandra Babcock, Capital Punishment, Mental Illness, and
Intellectual Disability: The Failure to Protect Individuals with Mental
Disorders Facing Execution, in United Nations Human Rights Office of the High
Commissioner, Death Penalty and the Victims (2016), available at https://www.ohchr.org/EN/newyork/Documents/Death-Penalty-and-the-Victims-WEB.PDF
>.
[77] See Margaret Hayes, The
Life Pattern of Incarcerated Women: The Complex and Interwoven Lives of Trauma,
Mental Illness, and Substance Abuse, 11 J. Forensic Nursing 214 (2015); United
States Department of Justice, Women’s Pathways to Jail: The Roles and
Intersections of Serious Mental Illness and Trauma (2012), available at
https://bja.ojp.gov/sites/g/files/xyckuh186/files/Publications/Women_Pathways_to_Jail.pdf
>; Marie Karlsson & Melissa Zielinski, Sexual Victimization and Mental
Illness Prevalence Rates Among Incarcerated Women: A Literature Review, 21
Trauma, Violence & Abuse 326 (2020).
[78] Id.
[79] Rebecca M. Shansky, Sex Differences
in PTSD Resilience and Susceptibility: Challenges for Animal Models of Fear
Learning, 1 Neurobiology of Stress 60, 60 (2014), available at
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4340080/
[80] 1.5 million women in the United
States face rape or physical abuse by an “intimate partner” annually;
additionally, over 50% of women have faced assault generally. More than three
million children witness domestic violence annually in the United States.
See Women in Prison Project, Survivors of Abuse Fact Sheet, 2009
(citing Extent, Nature and Consequences of Intimate Partner Violence, U.S.
Department of Justice, available at
http://www.ncdsv.org/images/WIPP_Suvivors_of_Abuse_Fact_Sheet_4-1-2009.pdf
>; National Institute of Justice (2000), National Violence Against Women
Survey, conducted by the U.S. Department of Justice and the U.S. Department of
Health and Human Services (1998), and Mary Kenning, Anita Merchant and Alan
Tomkins, Research on the Effects of Witnessing Parental Battering: Clinical
and Legal Policy Implications, in Women Battering: Policy Implications, ed.
Michael Steinman (Cincinnati: Anderson Publishers, 1991)).
[81] For example, one study in the U.S.
found that 57.3% of LGBTQ+ youth reported sexual harassment at school, 22.9% of
transgender students reported that they have experienced sexual dating violence,
35.5% of LGBTQ youth experience child sexual abuse, and 24% of LGBTQ youth had
engaged in some form of commercial sex in exchange for shelter, food, money, or
being sexually exploited by a third party. The National Child Traumatic Stress
Network, Identifying the Intersection of Trauma and Sexual Orientation and
Gender Identity, available at
https://www.nctsn.org/sites/default/files/resources/special-resource/identifying-the-intersection-of-trauma-and-sexual-orientation-and-gender-indentity-key-considerations.pdf
>. In another study, LGBTQ+ women of color experience greater exposure to
interpersonal potentially traumatic events and shame than white participants.
Scheer, J.R., Harney, P., Esposito, J., & Woulfe, J.M. (2019).
Self-reported mental and physical health symptoms and potentially traumatic
events among lesbian, gay, bisexual, transgender, and queer individuals: The
role of shame. Psychology of Violence, available at https://doi.apa.org/doiLanding?doi=10.1037%2Fvio0000241
[82] World Health Organization, Violence
against Women Fact Sheet, available at
https://www.who.int/news-room/fact-sheets/detail/violence-against-women
>. See also UN Women, Facts and Figures: Ending Violence Against
Women, available at https://www.unwomen.org/en/what-we-do/ending-violence-against-women/facts-and-figures(explaining that “an estimated 736 million women—almost
one in three—have been subjected to intimate partner violence, non-partner
sexual violence, or both at least once in their life.”).
[83] Vivianne Mbaku, Trauma-Informed
Lawyering, National Center on Law & Elder Rights, 1, available at
https://ncler.acl.gov/Files/Trauma-Informed-Lawyering.aspx
[84] Dale Vernor, PTSD is More Likely in
Women than Men, National Alliance on Mental Illness, (Oct. 8, 2019), available
at
https://www.nami.org/Blogs/NAMI-Blog/October-2019/PTSD-is-More-Likely-in-Women-Than-Men
>.
[85] See Women in Prison
Project, Survivors of Abuse Fact Sheet (2009), available at
http://www.ncdsv.org/images/WIPP_Wome_in_Prison_Fact_Sheet_4-2009.pdf(citing Prior Abuse Reported by Inmates and Probationers, Bureau of
Justice Statistics, U.S. Department of Justice, 2, (April 1999); Doris J.
James, Profile of Jail Inmates, 2002, Bureau of Justice Statistics, 10, U.S.
Department of Justice (July 2004), available at https://bjs.ojp.gov/content/pub/pdf/pji02.pdf
[86] See Women in Prison
Project, Survivors of Abuse Fact Sheet (2009) (citing Browne, Miller and Maguin,
Prevalence and Severity of Lifetime Physical and Sexual Victimization among
Incarcerated Women, 22 Int’l J. L. & Psych. 1, 3–4 (1999)), available at
http://www.ncdsv.org/images/WIPP_Suvivors_of_Abuse_Fact_Sheet_4-1-2009.pdf
>
[87] Lori Haskell, Women, Abuse and
Trauma Therapy: An Information Guide for Women and Their Families, Centre for
Addiction and Mental Health, (2004), available at
https://www.camh.ca/-/media/files/guides-and-publications/women-and-abuse-en.pdf?la=en&hash=F9DB2AC73F71A7F651727409004FFA211DEAF9A7
>.
[88] Id.
[89] Joan Cook, Past Trauma Causes Many
Women to Wind Up in Jail, The Hill (Dec. 6, 2018), available at
https://thehill.com/opinion/criminal-justice/420068-past-trauma-causes-many-women-to-wind-up-in-jail
>.
[90] Shannon M. Lynch, Ph.D., et al.,
Women’s Pathways to Jail: The Roles & Intersections of Serious Mental
Illness & Trauma, U.S. Dep’t of Justice, Bureau of Justice Assistance,
(2013), available at
https://bja.ojp.gov/sites/g/files/xyckuh186/files/Publications/WomensPathwaysToJail.pdf
>
[91] See Melissa S. Jones et
al., Life As She Knows It: The Effects Of Adverse Childhood Experiences On
Intimate Partner Violence Among Women Prisoners, 85 Child Abuse & Neglect
68, 68 (2018).
[92] Kylie Rymanowicz, Adverse Childhood
Experiences (ACEs): What Are They and How Can They Be Prevented?, Michigan State
University,
https://www.canr.msu.edu/news/adverse-childhood-experiences#:~:text=ACEs%20are%20divided%20into%20three,separation%2C%20divorce%20or%20substance%20abuse
>; American Academy of Pediatrics, Adverse Childhood Experiences and the
Lifelong Consequences of Trauma, 2, https://www.aap.org/en-us/documents/ttb_aces_consequences.pdf; see also Emily
M. Zarse, Mallory R. Neff, Rachel Yoder, Leslie Hulvershorn, Joanna E.
Chambers & R. Andrew Chambers, The Adverse Childhood Experiences
Questionnaire, 6 Cogent Medicine 1, 4 (2019).
[93] American Academy of Pediatrics,
Adverse Childhood Experiences and the Lifelong Consequences of Trauma, 2,
available at https://www.aap.org/en/patient-care/trauma-informed-care/
[94] Melissa S. Jones et al., Life As She
Knows It: The Effects Of Adverse Childhood Experiences On Intimate Partner
Violence Among Women Prisoners, 85 Child Abuse & Neglect 68, 69 (2018).
[95] Human Rights Project for Girls,
Georgetown Law Center on Poverty and Inequality, Ms. Foundation for Women, The
Sexual Abuse to Prison Pipeline, 9, available at
https://www.law.georgetown.edu/poverty-inequality-center/wp-content/uploads/sites/14/2019/02/The-Sexual-Abuse-To-Prison-Pipeline-The-Girls%E2%80%99-Story.pdf
>.
[96] Melissa S. Jones et al., Life As She
Knows It: The Effects Of Adverse Childhood Experiences On Intimate Partner
Violence Among Women Prisoners, 85 Child Abuse & Neglect 68, 76 (2018).
[97] Id.
[98] Studies in African, Asian, and Latin
American countries have demonstrated similar connections between ACEs and poor
health outcomes. Additionally, the prevalence of ACEs may be higher in low- and
middle-income countries. See Robert Wm Blum et al., Measuring Adverse
Child Experiences Among Young Adolescents Globally: Relationships
with Depressive Symptoms and Violence Perpetration, 65 Journal of
Adolescent Health 86, 86–87 (2019).
[99] The Harvard Trauma Questionnaire
(“HTQ”) is another useful tool for cross-cultural evaluation of trauma and its
unique symptomology. The Harvard Program in Refugee Trauma created six versions:
the Vietnamese, Cambodian, and Laotian versions to use with Southeast Asian
refugees, a Japanese version for 1995 Kobe earthquake survivors, a Croatian
version for soldiers who survived the violence in former Yugoslavian war, and a
Bosnian version for civilian survivors of that conflict. Further information on
the HTQ is available at
http://hprt-cambridge.org/screening/harvard-trauma-questionnaire/
>.
[100] Lori Haskell, Women, Abuse and
Trauma Therapy: An Information Guide for Women and Their Families, Centre for
Addiction and Mental Health, 1-2, available at
https://www.camh.ca/-/media/files/guides-and-publications/women-and-abuse-en.pdf?la=en&hash=F9DB2AC73F71A7F651727409004FFA211DEAF9A7
>
[101] Id.
[102] Id.
[103] See Lynch,
supra.
[104] See Vernor,
supra.
[105] See, e.g., Andrea L.
Roberts, et al., Pervasive Trauma Exposure Among US Sexual Orientation Minority
Adults and Risk of Posttraumatic Stress Disorder, American Journal of Public
Health (Dec 2010), available at
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2978167/ (Finding that the onset
of PTSD was higher among lesbians and gays, bisexuals, and heterosexuals with
any same-sex partners than it was among the heterosexual reference group,
which was largely “accounted for by sexual orientation minorities’ greater
exposure to violence, exposure to more potentially traumatic events, and
earlier age of trauma exposure.”).
[106] Susan Hatters Friedman, PTSD
Behind Bars: Incarcerated Women and PTSD, 3, (2015)
https://link.springer.com/content/pdf/10.1007%2F978-3-319-08613-2_57-1.pdf
>.
[107] See Vernor,
supra.
[108] Id. at 3-4.
[109] See Haskell,
supra.
[110] Center for Substance Abuse
Treatment (US), Trauma-Informed Care in Behavioral Health Services (2014),
Chapter 3: Understanding the Impact of Trauma, available at
https://www.ncbi.nlm.nih.gov/books/NBK207191/.
[111] Id.
[112] Bethany L. Brand et al.,
Assessing Trauma-Related Dissociation in Forensic Contexts: Addressing
Trauma-Related Dissociation as a Forensic Psychologist, Part II, 10
Psychological Injury and Law 298, 300 (2017).
[113] Id. at 303.
[114] Id.
[115] Id.
[116] Id. at 407.
[117] Id. at 412.
[118] See section above entitled
“Common Symptoms of Trauma.”
[119] Deborah Epstein & Lisa A.
Goodman, Discounting Women: Doubting Domestic Violence Survivors’ Credibility
and Dismissing Their Experiences, 167 University of Pennsylvania Law Review.
399, 410–411, 420 (2019), available at
https://www.pennlawreview.com/wp-content/uploads/2020/04/167-U-Pa-L-Rev-399.pdf
>
[120] See section above entitled
“Common Symptoms of Trauma.”
[121] Deborah Epstein & Lisa A.
Goodman, Discounting Women: Doubting Domestic Violence Survivors’ Credibility
and Dismissing Their Experiences, 167 University of Pennsylvania Law
Review. 399, 411 (2019), available at https://www.pennlawreview.com/wp-content/uploads/2020/04/167-U-Pa-L-Rev-399.pdf
>.
[122] Id.
[123] Id.
[124] Id. at 415–16.
[125] Id. at 414.
[126] Id.
[127] Id. at 416–17.
[128] Id.
[129] Id.
[130] Id. at 421.
[131] Mary Malefyt Seighman, Erika
Sussman, Olga Trujillo, Representing Domestic Violence Survivors Who Are
Experiencing Trauma and Other Mental Health Challenges: A Handbook for
Attorneys, National Center on Domestic Violence, Trauma & Mental Health 1,
15, (2011), available at
http://www.nationalcenterdvtraumamh.org/wp-content/uploads/2012/01/AttorneyHandbookMay282012.pdf
>
[132] Id.
[133] See Epstein &
Goodman, supra note 118, at 421.
[134] Id.
[135] Id.
[136] Id. at 422.
[137] See Kim E. Drake et al.,
Gender Differences in the Interplay Between Exposure to Trauma and Parental
Disturbances Within the Home, Stress-Sensitivity and Reported False Confessions
in Adolescents, 87 Personal and Individual Differences 282 (2015); Dr. Lenore
Walker, False Confessions of Women, Research, available at
http://www.drlenoreewalker.com/wp-content/uploads/2017/11/False-Confessions-Research.pdf
>.
[138] Id. at 286.
[139] Id.
[140] Walker, supra.
[141] Id.
[142] See Epstein &
Goodman, supra.
[143] Regina A. Schuller, The Impact of
Battered Women Syndrome Evidence on Jury Decision Process, 16 Law & Human
Behavior 597, 616 (1992).
[144] Bethany L. Brand et al.,
Assessing Trauma-Related Dissociation in Forensic Contexts: Addressing
Trauma-Related Dissociation as a Forensic Psychologist, Part I, 10 Psychological
Injury and Law 283, 291 (2017), available at
https://www.researchgate.net/profile/Bethany-Brand/publication/321945126_Assessing_Trauma-Related_Dissociation_in_Forensic_Contexts_Addressing_Trauma-Related_Dissociation_as_a_Forensic_Psychologist_Part_II/links/5a4cfa3faca2729b7c8b0eea/Assessing-Trauma-R
>.
[145] Kathleen J. Ferraro & NoÎl
Bridget Busch-Armendariz, The Use of Expert Testimony on Intimate Partner
Violence, VAWnet: The National Online Resource Center on Violence against Women
National Resource Center on Domestic Violence (NRCDV), available at
https://vawnet.org/material/use-expert-testimony-intimate-partner-violence
>.
[146] Id.
[147] Id.
[148] See id.
[149] Bethany L. Brand et al.,
supra.
[150] University of Sydney, Grounding
Techniques, 2, available at
https://www.sydney.edu.au/content/dam/students/documents/counselling-and-mental-health-support/grounding-techniques.pdf
>.
[151] Id.
[152] Katherine Stone, Debra Gindorf,
Postpartum Psychosis Sufferer Who Killed Her Kids, Gets Sentence Commuted,
Postpartum Progress, available at
https://postpartumprogress.com/debra-gindorf-postpartum-psychosis-sufferer-who-killed-her-kids-gets-sentence-commuted(last visited July 13, 2021)
[153] See Christina
Perez-Tineo, Criminal Prosecution and the Postpartum Period: A Call for More
Effective Application for the Insanity Defense 28 Annals Health Law Advance
Directive 203, 213-14 (2019).
[154] Id. at 213.
[155] Bridget F. Hutchens et al., Risk
Factors for Postpartum Depression: An Umbrella Review 65 Journal of Midwifery
Women’s Health 96, 96 (2020).
[156] Id. at 96.
[157] Id.
[158] Id. at 98.
[159] Terri Pearlstein et al.,
Postpartum Depression 200 American Journal of Obstetrics & Gynecology 357,
358 (2009).
[160] Perez-Tineo, supra.
[161] Pearlstein, supra.
[162] Id.
[163] Id.
[164] Id. at 211.
[165] See, e.g., Melissa L.
Nau, et al., 43 Postpartum Psychosis and the Courts 12, (2012) available at
http://jaapl.org/content/jaapl/40/3/318.full.pdf, Otty Sanchez, (2009) (found
not guilty by reason of insanity); Shontelle Cavanaugh (2010 (not guilty by
reason of insanity); Michelle Remington, (not guilty by reason of insanity
after four psychiatrists agreed that she suffered from postpartum
psychosis).
[166]See, e.g., H.G.
Virupaksha, Daliboyina Muralidhar, and Jayashree Ramakrishna, Suicide and
Suicidal Behavior among Transgender Persons (Nov-Dec 2016), available at
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5178031/ (reviewing studies of
suicide and suicidal behavior across countries and finding that 50% of
transgender persons in India have attempted suicide at least once before their
20th birthday, 50% of transgender persons in Australia have attempted suicide
at least once, and 48% of transgender youth in England had attempted suicide
at least once); Andrea L. Roberts, S. Bryn Austin, Heather L. Corliss, Ashley
K. Vandermorris, Karestan C. Koenen, Pervasive Trauma Exposure Among US Sexual
Orientation Minority Adults and Risk of Posttraumatic Stress Disorder,
American Journal of Public Health (Dec 2010), available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2978167/ (Finding that the onset
of PTSD was higher among lesbians and gays, bisexuals, and heterosexuals with
any same-sex partners than it was among the heterosexual reference group,
which was largely “accounted for by sexual orientation minorities’ greater
exposure to violence, exposure to more potentially traumatic events, and
earlier age of trauma exposure.”); Noah Adams, Ben Vincent, Suicidal Thoughts
and Behaviors Among Transgender Adults in Relation to Education, Ethnicity,
and Income: A Systematic Review, Transgender Health (Oct. 2019), available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6798808/ (finding that across
all projects reviewed suicide ideation among transgender individuals averaged
46.55% and of all transgender respondents, those who identified as First
Nations individuals had the highest rate of suicidal thoughts and behaviors,
followed by biracial/multiracial individuals, Black/African Americans,
Hispanics, Asian/Pacific Islanders, and Caucasians, which is attributable to
“colonization-based trauma”); Janko Jankovic, Vesna Slijepcevic, Vladimir
Miletic, Depression and suicidal behavior in lesbian, gay, bisexual and
heterosexual populations in Serbia and their differences: Cross-sectional
study, PLoS One (2020), available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7279590/.
[167] World Health Organization, Gender
and women’s mental health, available at
https://www.who.int/teams/mental-health-and-substance-use/gender-and-women-s-mental-health
>
[168]See, e.g. World Health
Organization, Breaking Barriers: Towards More Gender-Responsive and Equitable
Health Systems, at 26 (2019), available at
https://www.who.int/publications/m/item/breaking-barriers-towards-more-gender-responsive-and-equitable-health-systems(explaining that “LGBTI individuals face multiple and unique barriers to
health care” and “[h]ealth disparities are likely caused by marginalization,
stigma, and discrimination in society and health care systems, resulting in
chronic stress, poorer mental and physical health, and reluctance to seek
health services for fear of disrespect and discrimination or refusal of
services); id. (reporting that transgender persons experience a high rate of
mental health disorders, STIs, and substance abuse, but that “criminalization
and punitive laws against transgender people and sex workers . . . create
further roadblocks and disincentives for them to access health care”); id. at
7 (“women’s social independence influences access to health services”).
[169] World Health Organization, Gender
and women’s mental health, available at
https://www.who.int/teams/mental-health-and-substance-use/gender-and-women-s-mental-health
> (last date accessed 9/22/2021)
[170] National Institute of Mental
Health, Schizophrenia, available at
https://www.nimh.nih.gov/health/statistics/schizophrenia
(last date accessed 9/22/2021)</u >
[171] Leung M.D., D.A. and Chue M. R.
C. Psych., D.P. (2000), Sex differences in schizophrenia, a review of the
literature. Acta Psychiatrica Scandinavica, 101, 5, available at
https://doi.org/10.1111/j.0065-1591.2000.0ap25.x
[172] Id. at 6 citing Goldstein JM,
Santangelo SL, Simpson JC, Tsuang MT. The role of gender in identifying subtypes
of schizophrenia: a latent class analytic approach. Schizophr Bull.
1990;16(2):263-75, available at
https://pubmed.ncbi.nlm.nih.gov/2374884/
[173] Id at 6 citing Marneros A.
Frequency of occurrence of Schneider’s first rank symptoms in Schizophrenia. Eur
Arch Psychiatry Neurol Sci. 1984;234(1):78-82, available at
https://pubmed.ncbi.nlm.nih.gov/6489400/
[174] Gender Differences in Incidence
and Age at Onset of Mania and Bipolar Disorder Over a 35-Year Period in
Camberwell, England, Noel Kennedy et al., American Journal of
Psychiatry 2005 162:2, 259 available at
https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.162.2.257#R1622BHFFCCIB
>
[175] See e.g., Psychotic disorders in
women. (2016). In D. Castle & K. Abel (Eds.), Comprehensive Women’s Mental
Health, 269-347, Cambridge: Cambridge University Press, available at
https://doi.org/10.1017/CBO9781107045132.022 (discussing studies on gender
differences related to onset of Bi-Polar disorder); See also, Viguera, A.
C., Baldessarini, R. J., and Tondo, L. (2001). Response to lithium maintenance
treatment in bipolar disorders: Comparison of women and men. Bipolar
Disorders, 3, 245–252, available at
https://pubmed.ncbi.nlm.nih.gov/11903207/
[176] Kapfhammer, Hans-Peter. “Somatic
symptoms in depression.” Dialogues in clinical neuroscience vol. 8, 2 (2006)
227-239, available at
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181769/
[177] Samulowitz, Anke et al. “”Brave
Men” and “Emotional Women”: A Theory-Guided Literature Review on Gender Bias in
Health Care and Gendered Norms towards Patients with Chronic Pain.” Pain
research & management vol. 2018 6358624. (25 Feb. 2018), available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5845507/
[178] Progress in Mind, Psychiatry
& Neurology Resource Center (Sep. 14, 2020), Addressing the gender bias in
mental health research, available at
https://progress.im/en/content/addressing-gender-bias-mental-health-research
>
[179] Committee on the Elimination of
Discrimination Against Women, General Recommendation No. 35 on Gender-Based
Violence Against Women, UN Doc CEDAW/C/GC/35 (2017), available at
https://tbinternet.ohchr.org/Treaties/CEDAW/Shared%20Documents/1_Global/CEDAW_C_GC_35_8267_E.pdf
>
[180] World Health Organization,
Violence Against Women, available at
https://www.who.int/health-topics/violence-against-women#tab=tab, last
accessed Sep. 22, 2021.
[181] WHO, Violence Against Women: Key
Facts, available at
https://www.who.int/news-room/fact-sheets/detail/violence-against-women
>,last accessed Sep. 22, 2021.
[182] Michele R. Decker et al., “You Do
Not Think of Me as A Human Being”: Race and Gender Inequities Intersect to
Discourage Police Reporting of Violence Against Women, 96 J. Urban Health 772,
773 (2019) (United States); EU Agency for Fundamental Rights, Violence Against
Women, An EU Wide Survey: Main Results (2012) (Europe) available at
https://fra.europa.eu/sites/default/files/fra_uploads/fra-2014-vaw-survey-main-results-apr14_en.pdf
>.
[183] For example, in the U.S., nearly
50% of transgender people have been sexually assaulted in their lives. James, S.
E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M., The
Report of the 2015 U.S. Transgender Survey (2016), available at
https://www.transequality.org/sites/default/files/doc
s/USTS-Full-Report-FINAL.PDF.
[184] Leigh Goodmark, Should Domestic
Violence Be Decriminalized, 40 Harvard Women’s Law Journal. 53, 71 (2017).
[185] The Sentencing Project, Women and
Girls Serving Life Sentences (July 3, 2019), available at
https://www.sentencingproject.org/publications/women-girls-serving-life-sentences/.
>
[186] See Penal Reform
International, Women Who Kill in Response to Domestic Violence: How Do Criminal
Justice Systems Respond? (2016); Women in Prison Project, Survivors of Abuse
Fact Sheet (2009) available at
http://www.ncdsv.org/images/WIPP_Suvivors_of_Abuse_Fact_Sheet_4-1-2009.pdf
>; Christine A. Grant, Women Who Kill: The Impact of Abuse, 16 Issues in
Mental Health Nursing 315 (1995).
[187] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 64, NYU Press (2012).
[188] Shannon M. Lynch et al., Women’s
Pathways to Jail: The Role and Intersections of Serious Mental Illness and
Trauma, Bureau of Justice Assistance, U.S. Department of Justice (September
2012).
[189] See Leigh Goodmark, The
Impact of Prosecutorial Misconduct, Overreach, and Misuse of Discretion on
Gender Violence Victims, 123 Dickinson Law Review 627, 644-50 (2019).
[190] International Criminal Tribunal
for Rwanda, The Prosecutor v. Akayesu, Judgement, Case No. 96-4-T, ¶ 598 (2
September 1998). See also International Committee of the Red Cross, Rule 93:
Rape and Other Forms of Sexual Violence, available at
https://ihl-databases.icrc.org/customary-ihl/eng/docs/v1_rul_rule93
>.
[191] International Criminal Tribunal
for the Former Yugoslavia, Prosecutor v. Kunarac et al., Judgement, Case No.
IT-96-23, ¶ 438, (22 February 2001).
[192] Safe Lives, Psychological Abuse,
available at
https://safelives.org.uk/psychological-abuse.
[193] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 31-33, NYU Press (2012).
[194] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 33, NYU Press (2012).
[195] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 73, NYU Press (2012).
[196] Deborah Weissman, The Personal Is
Political—and Economic: Rethinking Domestic Violence, 2007 BYU Law Review 387,
389 (2007).
[197] Michele R. Decker et al., “You Do
Not Think of Me as A Human Being”: Race and Gender Inequities Intersect to
Discourage Police Reporting of Violence Against Women, 96 Journal of Urban
Health 772, 773 (2019).
[198] Under international law, a child
is a person below the age of 18. See UN Convention on the Rights of the
Child, Article 1.
[199] U.N. Committee on the Rights of
the Child, General Comment No. 13: The Right of the Child to Freedom from All
Forms of Violence, U.N. Doc. CRC/C/GC/13 ¶¶ 16, 29, 72 (2011). See also Article
21 of the African Charter on the Rights and Welfare of the Child, which
prohibits child marriage because of the harm it causes, and Articles 19 and 34
of the U.N. Convention of the Rights of the Child, which prohibit violence
against children and protect children from sexual abuse.
[200] APDF et al. v. Mali, App. No.
046/2016, Afr. Ct. H.P. Rights, ¶¶ 71–78 (2018).
[201] See generally Nawal M.
Nour, Health Consequences of Child Marriage in Africa, 12 Emerging Infectious
Diseases 1644 (2006) available at
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3372345/.
[202] Id.
[203] Commonwealth Secretariat,
Judicial Bench Book on Violence Against Women in Commonwealth East Africa, 289
(2017).
[204] Between January 1, 2008 and
September 30, 2020, there were 3,664 reported murders of transgender people
worldwide, 82% of which occurred in Central and South America. Transrespect
Versus Transphobia Worldwide, Press Release, available at
https://transrespect.org/wp
content/uploads/2020/11/TvT_TMM_TDoR2020_PressRelease_EN.pdf
[205] Trans Murder Monitor Update,
Trans Day of Remembrance 2020 (Nov. 11, 2020), available at
https://transrespect.org/en/tmm-update-tdor-2020/.
[206] Id.
[207] UN General Assembly, Convention
on the Rights of Persons with Disabilities: General Comment No. 3 on women and
girls with disabilities, 3-6, Nov. 25 2016, U.N. doc. CRPD/C/GC/3, available
at https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/Download.aspx?symbolno=CRPD/C/GC/3&Lang=en
>.
[208] See International
Criminal Tribunal for Rwanda, The Prosecutor v. Akayesu, Judgement, Case No.
96-4-T, ¶ 598 (2 September 1998); International Committee of the Red Cross, Rule
93: Rape and Other Forms of Sexual Violence, available at
https://ihl-databases.icrc.org/customary-ihl/eng/docs/v1_rul_rule93
>.
[209] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 43, NYU Press (2012).
[210] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 43, NYU Press (2012).
[211] In Indonesia, for example,
“corrective rape” occurs where women are “forced to have sex with a man to cure
them.” International Gay and Lesbian Human Rights Commission Summary Report,
Violence on the Basis of SOGI Against Non Heternormative Women in Asia (Feb.
2010), available at
https://outrightinternational.org/sites/default/files/386-1_0.pdf
>.
[212] In China, one study reported that
50% of lesbians faced family violence and 90% of lesbians above the age of 25
were forced to marry. International Gay and Lesbian Human Rights Commission
Summary Report, Violence on the Basis of SOGI Against Non Heternormative Women
in Asia (Feb. 2010), available at
https://outrightinternational.org/sites/default/files/386-1_0.pdf
>.
[213] Human Rights Watch, Japan, New
Momentum to Reform Transgender Law (May 25, 2021), available at
https://www.hrw.org/news/2021/05/25/japan-new-momentum-reform-transgender-law
>.
[214] As of 2021, seventy countries
have national laws criminalizing same sex conduct. Human Rights Watch, Outlawed:
“The Love That Dare Not Speak Its Name,” available at
http://internap.hrw.org/features/features/lgbt_laws/. Additionally, several
emirates criminalize same sex conduct in their own penal codes, including Abu
Dhabi, Dubai, and Sharjah, as well as the semi-autonomous Aceh province in
Indonesia, which criminalizes same-sex conduct under Sharia. And in 11 states
of the United States, unenforceable laws prohibiting consensual same-sex
conduct remain on the books despite a 2003 Supreme Court decision that found
such laws unconstitutional.
[215] See, e.g., Lakshmi
Gandhi, In Many Asian Languages, ‘LGBTQ’ doesn’t translate. Here’s how some fill
the gaps.” NBC News (Oct. 10, 2020), available at
https://www.nbcnews.com/news/asian-america/many-asian-languages-lgbtq-doesn-t-translate-here-s-how-n1242314
>.
[216] See, e.g., International Gay and
Lesbian Human Rights Commission Summary Report, Violence on the Basis of SOGI
Against Non Heternormative Women in Asia (Feb. 2010), available at
https://outrightinternational.org/sites/default/files/386-1_0.pdf
>.
[217] See, e.g., Rape Crisis
Center, Feelings & Stages Following Sexual Assault, available at
https://thercc.org/get-support/after-an-assault/feelings-stages-following-sexual-assault/
>; Washington Coalition of Sexual Assault Programs, The Effects of Sexual
Assault, available at https://www.wcsap.org/help/about-sexual-assault/effects-sexual-assault
>; Washington University in St. Louis, Rape Trauma Syndrome,
available at https://students.wustl.edu/rape-trauma-syndrome/.
[218] See International Gay
and Lesbian Human Rights Commission Summary Report, Violence on the Basis of
Sexual Orientation and Gender Identity Against Non Heternormative Women in Asia
(Feb. 2010), available at
https://outrightinternational.org/sites/default/files/386-1_0.pdf, Human
Rights Watch, Every Day I Live in Fear, Violence and Discrimination Against
LGBT People in El Salvador, Guatemala, and Honduras, and Obstacles to Asylum
in the United States, available at https://www.hrw.org/report/2020/10/07/every-day-i-live-fear/violence-and-discrimination-against-lgbt-people-el-salvador
>.
[219] Human Rights Watch, Every Day I
Live in Fear, Violence and Discrimination Against LGBT People in El Salvador,
Guatemala, and Honduras, and Obstacles to Asylum in the United States, available
at
https://www.hrw.org/report/2020/10/07/every-day-i-live-fear/violence-and-discrimination-against-lgbt-people-el-salvador
>.
[220] Leigh Goodmark, The Impact of
Prosecutorial Misconduct, Overreach, and Misuse of Discretion on Gender Violence
Victims, 123 Dickinson Law Review 627, 634 (2019), Leigh Goodmark, When Is a
Battered Woman Not a Battered Woman? When She Fights Back, 20 Yale Journal of
Law & Feminism 75, 83 (2008).
[221] Alisa Bierria & Colby Lenz,
Battering Court Syndrome: A Structural Critique of “Failure to Protect”, in The
Politicization of Safety 91, 91 (Jane Stoever ed., 2019).
[222] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 54, NYU Press (2012).
[223] Id.
[224] See generally Leigh
Goodmark, Should Domestic Violence Be Decriminalized, 40 Harvard Women’s Law
Journal. 53, 71-73 (2017).
[225] Michele R. Decker et al., “You Do
Not Think of Me As A Human Being”: Race and Gender Inequities Intersect to
Discourage Police Reporting of Violence Against Women, 96 Journal of Urban
Health 772, 773 (2019).
[226] See Incite!,
Gender Violence & Race, available at
https://incite-national.org/gender-violence-race/. As the researcher and
advocate Leigh Goodmark notes, “women of color have negative, even abusive,
experiences with police when they call for assistance with domestic violence.”
Leigh Goodmark, Should Domestic Violence Be Decriminalized, 40 Harvard Women’s
Law Journal. 53, 73 (2017).
[227] Michele R. Decker et al., “You Do
Not Think of Me As A Human Being”: Race and Gender Inequities Intersect to
Discourage Police Reporting of Violence Against Women, 96 Journal of Urban
Health 773, 772 (2019).
[228] In Mexico, for example, police
are the “primary predators” who target transgender women and subject them to
abuse, arbitrary arrest, and extortion. Transgender Law Center, Report on Human
Rights Conditions of Transgender Women in Mexico 18 (May 2016), available at
https://transgenderlawcenter.org/wp-content/uploads/2016/05/CountryConditionsReport-FINAL.pdf
>. According to a 2013 report by the Anti-Violence Project, transgender
people in the United States are 7 times more likely to experience physical
violence when interacting with police than cisgender victims and survivors.
Anti-Violence Project, Hate Violence Against Transgender Communities,
available at https://avp.org/wp-content/uploads/2017/04/ncavp_transhvfactsheet.pdf
>.
[229] The term “domestic violence” is
commonly used but is not perfect. Some critics argue that the word “domestic”
adds an unwarranted softness to the concept by reinforcing that such violence
happens in a family setting. Another common term is “intimate partner violence,”
but this term fails to encompass violence that occurs between non-intimate
partners, such as a parent’s violence towards their child. In this chapter, we
will refer to “domestic violence” because it is a prevalent term that is widely
recognized in legal systems. For an in-depth analysis of these critiques, see
Chapter Two: Defining Domestic Violence, in Leigh Goodmark, A Troubled Marriage:
Domestic Violence and the Legal System, 29–53, NYU Press (2012).
[230] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 33-34, NYU Press (2012)
[231] Rachel Louise Snyder, No Visible
Bruises: What We Don’t Know About Domestic Violence Can Kill Us, 5 (2019).
[232] Rachel Louise Snyder, No Visible
Bruises: What We Don’t Know About Domestic Violence Can Kill Us, 5 (2019).
[233] Michele R. Decker et al., “You Do
Not Think of Me As A Human Being”: Race and Gender Inequities Intersect to
Discourage Police Reporting of Violence Against Women, 96 Journal of Urban
Health 772, 773 (2019).
[234] Kae Greenberg, Still Hidden in
the Closet: Trans Women and Domestic Violence, 27 Berkeley J. of Gender, Law
& Justice 198, 200 (Summer 2012).
[235] Id. at 198.
[236] See Carolyn B. Ramsey,
The Exit Myth: Family Law, Gender Roles, and Changing Attitudes Toward Female
Victims of Domestic Violence, 20 Mich. J. Gender & L. 1, 6 (2013); Leigh
Goodmark, Should Domestic Violence Be Decriminalized, 40 Harv. Women’s L.J. 53,
61 (2017).
[237] See, e.g., CEDAW,
General Recommendation No. 35, ¶ 9; Maputo Protocol Article 4(a)); Opuz v.
Turkey, European Court of Human Rights, App. No. 33401/02, ¶¶ 96, 145 (2009).
[238] Rachel Louise Snyder, No Visible
Bruises: What We Don’t Know About Domestic Violence Will Kill Us, 36 (2019).
[239] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 42, NYU Press (2012).
[240] Id. at 35.
[241] Id.
[242] Id. at 36.
[243] Rachel Louise Snyder, No Visible
Bruises: What We Don’t Know About Domestic Violence Can Kill Us, 25 (2019).
[244] In the US, 75% of all domestic
homicides occur when the victim is trying to leave her abuser.
See Shelter for Help in Emergency, Why Doesn’t She Just Leave?,
available at
https://www.shelterforhelpinemergency.org/news-list/132-why-doesn-t-she-just-leave
>.
[245] Id.
[246] Leigh Goodmark, A Troubled
Marriage: Domestic Violence and the Legal System, 73, NYU Press (2012).
[247] Kae Greenberg, Still Hidden in
the Closet: Trans Women and Domestic Violence, 27 Berkeley Journal of Gender,
Law & Justice 198, 225 (Summer 2012).
[248] See also SVRI, Six
Golden Principles for Interviewing Women Who May Have Experienced Violence
(Sept. 6, 2017), available at
https://www.svri.org/blog/six-golden-principles-interviewing-women-who-may-have-experienced-violence
>.
[249] UNFPA et al., GBV Assessment
& Situation Analysis Tools (Feb. 2012), available at
https://www.refworld.org/pdfid/5c3465c64.pdf.
[250] Sexual Violence Research
Initiative, Six Golden Principles for Interviewing Women Who May Have
Experienced Violence (Sept. 6, 2017), available at
https://www.svri.org/blog/six-golden-principles-interviewing-women-who-may-have-experienced-violence
>.
[251] Asmita Ghosh, How to Sensitively
Interview Survivors Of Sexual Violence, Feminism in India (Nov. 26, 2019),
available at
https://feminisminindia.com/2019/11/26/sensitively-interview-survivors-gbv/
>.
[252] Id.
[253] WITNESS, Tips: Interviewing
Survivors of Gender-Based Violence (March 2017), available at
https://www.witness.org/new-tipsheet-interviewing-survivors-gbv/
>.
[254] Id.
[255] WITNESS, Conducting Safe,
Effective and Ethical Interviews with Survivors of Sexual and Gender-Based
Violence, 6-7, available at
https://s3-us-west-2.amazonaws.com/librarywebfiles/Training+Materials/Training+PDFs/Guide+to+Interviewing+Survivors+of+Gender-Based+Violence/English/Conducting-Safe-Effective-and-Ethical-Interviews-with-Survivors-of-Sexual-and-Gender-Based-Violence_v1.0.p
>.
[256] Id.
[257] WITNESS, Conducting Safe,
Effective and Ethical Interviews with Survivors of Sexual and Gender-Based
Violence, 6-7, available at
https://s3-us-west-2.amazonaws.com/librarywebfiles/Training+Materials/Training+PDFs/Guide+to+Interviewing+Survivors+of+Gender-Based+Violence/English/Conducting-Safe-Effective-and-Ethical-Interviews-with-Survivors-of-Sexual-and-Gender-Based-Violence_v1.0.p
>.
[258] Id. at 11.
[259] Id.
[260] RAINN, Tips for Interviewing
Survivors, available at
https://www.rainn.org/articles/tips-interviewing-survivors.
[261] For more information on signs of
distress and discomfort, read Chapter 3 of this manual, specifically the section
entitled Trauma.
[262] WITNESS, Conducting Safe,
Effective and Ethical Interviews With Survivors of Sexual and Gender-Based
Violence, 6-7, 11 available at
https://s3-us-west-2.amazonaws.com/librarywebfiles/Training+Materials/Training+PDFs/Guide+to+Interviewing+Survivors+of+Gender-Based+Violence/English/Conducting-Safe-Effective-and-Ethical-Interviews-with-Survivors-of-Sexual-and-Gender-Based-Violence_v1.0.p
>.
[263] Id.
[264] For a sample list of breathing
exercises and meditations see Chapter 3 on Trauma.
[265] RAINN, Tips for Interviewing
Survivors, available at
https://www.rainn.org/articles/tips-interviewing-survivors.
[266] Dara E. Purvis & Melissa
Blanco, Police Sexual Violence: Police Brutality, #MeToo, and Masculinities, 108
CALIFORNIA LAW REVIEW 5, (Oct. 2020), available at
https://www.californialawreview.org/print/police-sexual-violence/.
See also Mona El-Naggar, et al., When a Search Crosses the Line, NEW
YORK TIMES (Jul. 5, 2021), available at https://www.nytimes.com/interactive/2021/07/05/world/middleeast/egypt-sexual-assault-police.html
>.
[267] Dara E. Purvis & Melissa
Blanco, Police Sexual Violence: Police Brutality, #MeToo, and Masculinities, 108
CALIFORNIA LAW REVIEW 5, (Oct. 2020), available at
https://www.californialawreview.org/print/police-sexual-violence/.
>
[268] Neela Ghoshal, Uganda LGBT
Shelter Residents Arrested on COVID-19 Pretext, HUMAN RIGHTS WATCH (Apr. 3,
2020), available at
https://www.hrw.org/news/2020/04/03/uganda-lgbt-shelter-residents-arrested-covid-19-pretext
>.
[269] See, e.g., Dustin
Gardiner, California moves to repeal loitering law that trans activists say
leads to bias, SAN FRANCISCO CHRONICLE (Sept. 11, 2021) (discussing efforts to
repeal an anti-loitering law that “allows law enforcement to target transgender
women and women of color simply because of innocuous factors like how they dress
or where they stand on the street”).
[270] See, e.g., Christiana
Prater-Lee, #Justice4Layleen: The Legal Implications of Polanco v. City of New
York, 47 AM. J. OF LAW & MEDICINE 144, 148 (2021) (describing “walking while
trans” laws and their impact).
[271] See, e.g., Neela
Ghoshal, In Cameroon Transgender Women Given Five-Years in Prison, HUMAN RIGHTS
WATCH (May 12, 2021), available at
https://www.hrw.org/news/2021/05/12/cameroon-transgender-women-given-five-years-prison(explaining that in Cameroon, “security forces have increasingly targeted
people for arbitrary arrest based on their real or perceived sexual
orientation or gender identity”).
[272] See, e.g., Christy
Mallory, et al., Discrimination and Harassment by Law Enforcement Officers in
the LGBT Community, THE WILLIAMS INSTITUTE, 2 (Mar. 2015), available at
https://williamsinstitute.law.ucla.edu/wp-content/uploads/LGBT-Discrimination-by-Law-Enforcement-Mar-2015.pdf(citing a 2013 report finding that, in the U.S., “of the LGBT violence
survivors surveyed who interacted with police, 48% reported that they had
experienced police misconduct, including unjustified arrest, use of excessive
force and entrapment” and a 2012 report finding that 24% of Latina transgender
women in Los Angeles County had been sexually assaulted by law
enforcement).
[273] Human Rights Watch, Uganda: Stop
Police Harassment of LGBT People (Nov. 17, 2019), available at
https://www.hrw.org/news/2019/11/17/uganda-stop-police-harassment-lgbt-people
>.
[274] In February 2021 in Cameroon,
gendarmes arrested two transgender women for wearing typically female clothing,
“interrogated the women without a lawyer present, beat and threatened to kill
them, taunted them with anti-LGBT epithets, and forced them to sign statements…”
Neela Ghoshal, In Cameroon Transgender Women Given Five-Years in Prison, HUMAN
RIGHTS WATCH (May 12, 2021), available at
https://www.hrw.org/news/2021/05/12/cameroon-transgender-women-given-five-years-prison
>.
[275] Penal Reform International,
LGBTQ+ People: The Issue, available at
https://www.penalreform.org/issues/lgbtq-people/the-issue/.
[276] Dara E. Purvis & Melissa
Blanco, Police Sexual Violence: Police Brutality, #MeToo, and Masculinities, 108
CALIFORNIA LAW REVIEW 5, (Oct. 2020), available at
https://www.californialawreview.org/print/police-sexual-violence/
>.
[277] Gisli H. Gudjonsson, et al.,
False Confessions and Individual Differences: The Importance of Victimization
among Youth, 45 J. PERSONALITY & INDIVIDUAL DIFFERENCES 8, 804 (2008).
[278] Judith Herman, Trauma and
Recovery: The Aftermath of Violence—From Domestic Abuse to Political Terror,
BASIC BOOKS, 111 (1992).
[279] Lenore Walker, False Confessions
of Battered Women, The Battered Woman Syndrome, 4th ed., SPRINGER PUBLISHING
COMPANTY, 459 (2017).
[280] Michelle Bachelet, Death penalty
and gender dimension: Exploring disadvantage and systemic barriers affecting
death sentences, UN HUMAN RIGHTS COUNCIL (Sept. 24, 2020), available at
https://perma.cc/E7QQ-HSAB; Cornell Center on the Death Penalty Worldwide,
Judged for More Than Her Crime: A Global Overview of Women Facing the Death
Penalty, 6 (Sep. 2018).
[281] Marc Bookman, Sex Shamed to
Death: How Oklahoma Prosecutors Used Sex and Infidelity to Put a Woman on Death
Row, THE APPEAL (2017), available at
https://theappeal.org/sex-shamed-to-death-5a28cc7cf2fc/.
[282] State v. Pushpa, CIS No.
SC/134/2013, Supreme Ct. of India; National Law University Delhi Project 39A,
Research Report to the Cornell Center on the Death Penalty Worldwide, Nov. 8,
2017.
[283] Vaibhav Ganjapure, Six on death
row for ‘human sacrifice’ case move HC, THE TIMES OF INDIA (Aug. 4, 2018),
available at
http://timesofindia.indiatimes.com/articleshow/65264395.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst
>; Surender Sharma, HC upholds death sentence to Rohtak girl who killed 7
of her family, HINDUSTAN TIMES (Jul. 18, 2018), available at https://www.hindustantimes.com/punjab/hc-upholds-death-sentence-to-rohtak-girl-who-killed-7-of-her-family/story-pX3SlwDCPABoq3YLuN5EcK.html
>; Hindustan Times, Supreme Court stays couple’s execution in human
sacrifice case, HINDUSTAN TIMES (Aug. 17, 2017), available at https://www.hindustantimes.com/india-news/supreme-court-stays-couple-s-execution-in-human-sacrifice-case/story-k8AqSmGMgeMr4i8ozKVzQJ.html
>; Khojkhabarnews, 11 year son’s eyewitness account leads to death sentence
of mother, life term to her paramour (Dec. 6, 2016); The Hindu, Death sentence
upheld in Mumbai blasts case (Nov. 18, 2016), available at https://www.thehindu.com/news/national/Death-sentence-upheld-in-Mumbai-blasts-case/article13302108.ece
>; Uma Vishnu, Shabnam & Saleem: The relationship that claimed seven
lives of a family, THE INDIAN EXPRESS (Jun. 7, 2015), available at https://indianexpress.com/article/india/india-others/sunday-story-shabnam-saleem-the-amroha-murders/
>; The Times of India, Woman, two others get death for triple murder (Dec.
13, 2014), available at http://timesofindia.indiatimes.com/articleshow/27322790.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst
>; Mayura Janwalkar, The sons of a woman on death row, THE INDIAN EXPRESS
(Sept. 1, 2014), available at https://indianexpress.com/article/india/maharashtra/the-sons-of-a-woman-on-death-row/
>. We have no information on the case of one of the twelve women on death
row.
[284] LBH Masyarakat, Research Report
to the Cornell Center on the Death Penalty Worldwide, Sep. 25, 2017.
[285] Professor Kimberlé Crenshaw
coined the term “intersectionality” in her seminal essay, Demarginalizing the
Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination
Doctrine, Feminist Theory and Antiracist Politics. See Kimberlé Crenshaw,
Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of
Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics, 1989
UNIVERSITY OF CHICAGO LEGAL FORUM 1 (1989), available at
https://chicagounbound.uchicago.edu/cgi/viewcontent.cgi?article=1052&context=uclf
>.
[286] Racial discrimination in the
courtroom is well documented in the United States, for example.
See, e.g., Sheri L. Johnson, Racial Imagery in Criminal Cases, 67
TULANE LAW REVIEW 6 (1993); Jerry Kang, et al., Implicit Bias in the Courtroom,
59 UCLA LAW REVIEW 1124 (2012); Praatika Prasad, Implicit Racial Biases in
Prosecutorial Summations: Proposing an Integrated Response, 18 FORDHAM LAW
REVIEW 667 (2018); Ryan P. Alford, Appellate Review of Racist Summations:
Redeeming the Promise of Searching Analysis, 11 MICHIGAN JOURNAL OF RACE &
LAW 325 (2006).
[287] U.N. Committee on the Elimination
of Racial Discrimination, General Recommendation No. 25 on Gender Related
Dimensions of Racial Discrimination, U.N. Doc CERD/C/GC/25 (2000).
[288] Animal imagery is a prevalent
racist trope in the United States. For a fuller description of the racial
implications of such imagery and its use in capital cases, See Sheri L.
Johnson, Racial Imagery in Criminal Cases, 67 TULANE LAW REVIEW 6 (1993).
[289] Jack Britton, Capital Punishment,
Human Rights, and Indonesia’s Chance for the Moral High Ground, THE DIPLOMAT
(Apr. 3, 2018), available at
https://thediplomat.com/2018/04/capital-punishment-human-rights-and-indonesias-chance-for-the-moral-high-ground/
>; U.N. experts urge UAE to quash the death sentence against a woman
migrant domestic worker, UN HUMAN RIGHTS OFFICE OF THE HIGH COMMISSIONER (Mar.
30, 2017), available at https://www.ohchr.org/en/NewsEvents/Pages/DisplayNews.aspx?NewsID=21462&LangID=E
>.
[290] Anonymous Source, Interview with
the Cornell Center on the Death Penalty Worldwide.
[291] Anonymous Source, Interview with
the Cornell Center on the Death Penalty Worldwide; U.S. State Dept., United Arab
Emirates 2015 Human Rights Report, 4, 7, 8, available at
https://www.state.gov/documents/organization/253163.pdf, 2015.
[292] U.N. Office on Drugs and Crime,
Handbook on Women and Imprisonment (Mar. 2014), available at
https://www.unodc.org/documents/justice-and-prison-reform/women_and_imprisonment_-_2nd_edition.pdf
>.
[293] ICCPR Art. 14(3)(f); ACHR Art.
8(2)(a). ECHR, Art. 6(3)(e); CRC Art. 40(2)(vi). See also Amnesty
Intl., Fair Trial Manual, Second edition, POL 30/002/2014, 84 (Apr. 9, 2014).
[294] VCCR Art. 36(1)(b).
[295] European and South American
embassies tend to provide more assistance to their arrested nationals than
embassies from other countries. Malaysian officials are particularly unlikely to
notify embassies from African countries, and embassies from African countries
are especially unlikely to provide assistance to their arrested nationals.
See Carolyn Hoyle, Monash panel, Drug Offenses and the Death Penalty in
Malaysia, available at
https://perma.cc/2WUG-YLMN, May 28,
2020. Additionally, some foreign nationals belonging to targeted minorities in
their countries of origin receive less consular support. For example, embassies
provide varying levels of support for the pardon petition process. According to
reports, embassy representatives from the Filipino and Indonesian embassies help
many of their nationals seek a pardon, while foreign nationals from some African
and Middle Eastern countries, along with foreign nationals from targeted
minorities in their countries of origin, receive little or no support from their
embassies. See Amnesty Intl., Fatally Flawed: Why Malaysia Must Abolish
the Death Penalty, ACT 50/1078/2019, 32, 40 (Oct. 8, 2019).
[296] VCCR Art. 36(1)(b).
See also Amnesty Intl., Fair Trial Manual, Second edition, POL
30/002/2014, 84 (Apr. 9, 2014).
[297] Avena & Other Mexican
Nationals (Mex. v. United States), 2004 I.C.J. 128 (Mar. 31).
[298] See, e.g., Penal Reform
International and Thailand Institute of Justice, Global Prison Trends 2021 (May
2021), available at
https://cdn.penalreform.org/wp-content/uploads/2021/05/Global-prison-trends-2021.pdf(describing “new research specifically on trans women in Latin America
published in 2020 concluded from all the available data that trans women
represent a significant proportion of the LGBTQ+ population in prison,
exceeding 30 per cent in Mexico City and in Bolivia); Penal Reform
International, LGBTQ+ People: The Issue, available at https://www.penalreform.org/issues/lgbtq-people/the-issue/
(“Globally, lesbian, gay and bisexual detainees are in a situation of
particular vulnerability and at risk of human rights violations and abuses”
and “are over-represented in prison populations”); Alexi Jones, Visualizing
the Unequal Treatment of LGBTQ People in the Criminal Justice System (March 2,
2021), available at https://www.prisonpolicy.org/blog/2021/03/02/lgbtq/ (LGBTQ+ people “are
arrested, incarcerated, and subjected to community supervision at
significantly higher rates than straight and cisgender people” and “[t]his is
especially true for trans people and queer women” […] In the U.S., “40% of
girls (who were assigned female at birth) in the juvenile justice system
identify as LGBQ and/or gender nonconforming.”).
[299] Human Rights Watch, #Outlawed:
“The Love That Dare Not Speak Its Name,” available at
http://internap.hrw.org/features/features/lgbt_laws/
[300] Id. (At least 13 countries,
including Brunei, the Gambia, Indonesia, Jordan, Kuweit, Malawi, Malaysia,
Nigeria, Oman, Saudi Arabia, South Sudan, Tona, and the United Arab Emirates,
have laws that target transgender people and criminalize certain forms of gender
expression. For example, Brunei, Oman, and Kuwait have laws that criminalize
“posing as” or “imitating” a person of a different sex. Malaysia also
criminalizes “posing as” a different sex in the Sharia codes of each of its
states and its federal territory; Nigeria criminalizes transgender people in its
northern states under Sharia codes. While Saudi Arabia has no codified law,
police routinely arrest people based on their gender expression. In South Sudan
and Malawi, laws criminalizing gender identity and expression target transgender
women specifically. In South Sudan, the laws only apply to men who “dress as
women”; in Malawi, laws apply to men who wear their hair long. Tonga’s laws
target trans women who are sex workers, prohibiting any “male person” from
presenting as female while “soliciting for an immoral purpose, in a public place
with intent to deceive any other person as to his true sex.” The United Arab
Emirates has laws that prohibit men “posing as” women in order to enter
women-only spaces and the UAE has prosecuted transgender people under this law.)
[301] Christopher Alexander & Mai
Sato, State-Sanctioned Killing of Sexual Minorities: Looking Beyond the Death
Penalty (April 12, 2021), available at
https://deathpenaltyworldwide.org/state-sanctioned-killing-of-sexual-minorities-looking-beyond-the-death-penalty/(discussing the death penalty for same-sex acts, extrajudicial killings
encompassing “gay purges” and insurrectional movements,” conversion practices,
and lawful excuses for homicide across countries).
[302]
Alexi Jones, Visualizing the Unequal Treatment of LGBTQ People in the
Criminal Justice System (March 2, 2021), available at https://www.prisonpolicy.org/blog/2021/03/02/lgbtq/.
[303] National Center for Transgender
Equality, LGBTQ People Behind Bars: A Guide to Understanding the Issues Facing
Transgender Prisoners and Their Legal Rights, 5, available at
https://transequality.org/sites/default/files/docs/resources/TransgenderPeopleBehindBars.pdf
>.
[304] Id.
[305] Id.; see also Jerome
Hunt and Aisha C. Moodie-Mills, The Unfair Criminalization of Gay and
Transgender Youth (June 29, 2012) (“These higher rates of involvement in the
juvenile justice system are a result of gay and transgender youth abandonment by
their families and communities, and victimization in their schools . . . .).
[306] Joey L. Mogul, The Dykier, The
Butcher, The Better: The State’s Use of Homophobia and Sexism to Execute Women
in the United States, 8 NYC Law Review 473, 473-474, 487 (2005).
[307] Id. at 490.
[308] U.N. Office on Drugs and Crime,
Handbook on Women and Imprisonment, (2014), available at
https://www.unodc.org/documents/justice-and-prison-reform/women_and_imprisonment_-_2nd_edition.pdf
>, Mar. 2014
[309] Judy Fudge & Rosemary Owens,
Precarious Work, Women, and the New Economy: The Challenge to Legal Norms, 13,
Precarious Work, Women, and the New Economy: The Challenge to Legal Norms, Hart
Publishing, (Apr. 26, 2006).
[310] Lucy Harry, 10 Rethinking the
Relationship between Women, Crime and Economic Factors: The Case-Study of Women
Sentenced to Death for Drug Trafficking in Malaysia, Laws 9, 4, (Jan. 31, 2021).
[311] Sara Elder & Sriani Kring,
Young and Female – A Double Strike?, 36, Work4Youth Publication Series No. 32,
(Jan. 2016). (Employers in many countries have expressed a preference for hiring
men, and men tend to receive higher wages than women, including for the same
occupations). See Id. at 37, 40, Additionally, oppressive gender
discourses justify the segregation of women into menial work: in Malaysia, one
“[employer’s] strategy was underpinned by orientalist discourses where women are
considered not only to have naturally nimble fingers, but also to be naturally
more docile and willing to accept tough work discipline, and naturally less
inclined to join trade unions, than men; and to be naturally more suited to
tedious, repetitious, monotonous work.” See Lucy Harry,
supra note 309.
[312] Leonora C. Angeles & Sirijit
Sunanta, Demanding Daughter Duty: Gender, Community, Village Transformation, and
Transnational Marriages in Northeast Thailand, 549-574, Critical Asian Studies
41, no. 4, (Dec. 1, 2009). Fatima Khan, et al., Parental Modeling as Predictor
of Filial Obligation in Young Adults, 56, ResearchGate,
https://perma.cc/AZ4X-55M7, (Dec. 2017). A study based on interviews with
Indonesian youth suggests that women in Indonesia are expected to play a
dominant role in caring for elderly family members. See Rahmi
Setiyani and Carol Windsor, Filial Piety: From the Perspective of Indonesian
Young Adults, 51, 9 Nurse Media Journal of Nursing 1, ( Jun. 2019). A study
from Malaysia suggests that daughters are more involved in caring for elderly
parents than sons and that elderly parents expect more help/support from their
daughters than from their sons. See Khadijah Alavi & Rahim M.
Sail, Roles of Malay Women in the Process of Caring for Elderly Parents:
Dilemma and Challenges in the Era of Globalisation, 72–73, 28 Kajian Malaysia
2, (Jan. 1, 2010). A different study of 56 informal caregivers in Malaysia
concludes that females, especially daughters, are usually the informal
caregivers to elderly relatives. See Zheng-Yi et al., The Formal and
Informal Long-term Caregiving for the Elderly: the Malaysian Experience, 174,
9 Asian Social Science 4, (Mar. 28, 2013).
[313] Globally, 84.3% of one-parent
households are lone-mother households. See U.N. Women, Progress of the
World’s Women 2019-2020: Families in a Changing World, 63, available at
https://perma.cc/L54R-W5RJ, (Jun. 25, 2019).
[314] Id. at 129-130.
[315] The ECOWAS Court ruled that it
did not have competence to order Nigeria to vacate the death sentence. Instead,
it ordered a stay of execution.
Maimuna Abdulmumini v. Federal Republic of Nigeria, Kastina State Government,
and the Nigerian Prisons Service, Decision secs. 1–2, ECW/CCJ/jud/14/14,
Community Ct. of Justice, ECOWAS, Jun. 10, 2014.
[316] International Covenant on Civil
and Political Rights (ICCPR), Article 6.
[317] ICCPR, Article 6(5).
[318] Cornell Center on the Death
Penalty Worldwide, International Legal Issue: Women, (Jan. 25, 2012) available
at
https://deathpenaltyworldwide.org/publication/women/
[319] At least 50 states have adopted
legislation prohibiting the execution of mothers with young children, deriving
in large part by states’ concern for the welfare of innocent/small children.
Forty-one countries, for example, have acceded to the African Charter on the
Rights and Welfare of the Child, which prohibits the imposition of a death
sentence on mothers of infants and young children. See Sandra L.
Babcock, Deciding Who Lives And Who Dies: Eligibility for Capital Punishment
Under National and International Law, in United Nations Office of the High
Commissioner, Comparative Capital Punishment, 65 (2016).
[320] Prot. to the African Charter on
Human and People’s Rights on the Rights of Women in Africa, art. 4, OAU Doc.
CAB/LEG/66.6, Jul. 11, 2003.
[321] African Charter on the Rights and
Welfare of the Child, art. 30(e), OAU Doc. CAB/LEG/24.9/49, Jul. 11, 1990.
[322] Arab Charter on Human Rights,
art. 12, Sep. 15, 1994.
[323] Prot. to the African Charter on
Human and Peoples’ Rights on the Rights of Women in Africa, art. 4, OAU Doc.
CAB/LEG/66.6, Jul. 11, 2003. African Charter on the Rights and Welfare of the
Child, art. 30(e), OAU Doc. CAB/LEG/24.9/49, Jul. 11, 1990.
[324] Arab Charter on Human Rights,
art. 12, Sep. 15, 1994.
[325] See Sandra L. Babcock, Deciding
Who Lives and Who Dies: Eligibility for Capital Punishment Under National and
International Law, in United Nations Office of the High Commissioner,
Comparative Capital Punishment, Comparative Capital Punishment, 65 (2016).
[326] Human rights bodies recognize the
heightened risk of violence that some women face because of these intersecting
forms of discrimination. See Gonzales, Case 12,626, at ¶¶ 113 (“The
Commission has also recognized that certain groups of women face discrimination
on the basis of more than one factor during their lifetimes, based on their . .
. race and ethnic origin, among others, which increases their exposure to acts
of violence. Protection measures are considered particularly critical in [these
cases], since [these groups] may be at greater risk of human rights violations
based on two factors….”).
[327] Human rights bodies across the
world concur that gender-based violence is a form of impermissible gender
discrimination, including when violence is perpetuated in the home by a family
member. See Committee on the Elimination of Discrimination Against
Women (CEDAW),
General Recommendation No.35 on Gender-Based Violence Against Women,
U.N. Doc CEDAW/C/GC/35, ¶ 1 (2017) (hereinafter “CEDAW GR 35”); Office of the
High Commissioner for Human Rights Res. 2003/45, Elimination of Violence Against
Women (Apr. 23, 2003); Opuz v. Turkey, Eur. Ct. H.R., App. No.
33401/02, ¶¶ 184–89 (2009); Assembly of the African Union, Maputo Protocol, art.
3 (2003).
[328] UN Special Rapporteur, Due
Diligence Standard as a Tool for the Elimination of Violence Against Women
(2006).
[329] See CEDAW GR 35
(establishing that States must adopt positive measures to protect women’s right
to be free from gender-based violence); Belem do Para Convention, art. 7-8;
Istanbul Convention, art. 5; Maputo Protocol, art. 2(d).
[330] See Belem do Para
Convention, art. 7(c)-7(d) (requiring States to adopt legislative,
administrative, and legal measures to prevent violence against women); CEDAW GR
35.
[331] In many countries, medical
personnel have an obligation to report instances of gender-based violence of
which they become aware. In Tanzania, for example, medical staff have an
obligation to file Police Form 3, a medical examination report completed by both
law enforcement officers and medical practitioners which documents a victim’s
injuries. See Tanzania Police Force, Medical Examination Report,
available at
https://www.tanzania.go.tz/egov_uploads/documents/pf_3_form_sw.pdf
>. See also Human Rights Watch, Discrimination Against Sex
Workers, Sexual and Gender Minorities, and People Who Use Drugs in Tanzania,
75-78 (2013) (explaining the requirement for Police Form 3 and that underlying
rationale of this requirement is to enable law enforcement to effectively
investigate interpersonal violence).
[332] The UN Convention on the Rights
of the Child defines children as those under the age of 18. See UN
Convention on the Rights of the Child, art. 1.
[333] Inter-Am. Comm’n, Violence and
Discrimination Against Women and Girls, ¶ 11.
[334] U.N. Committee on the Rights of
the Child, General Comment No. 13: The Right of the Child to Freedom from All
Forms of Violence, U.N. Doc. CRC/C/GC/13 ¶¶ 16, 29, 72 (2011). Much regional
jurisprudence reiterates that child marriage is a harmful practice in violation
of girls’ human rights. See, e.g., APDF et al. v. Mali, App. Mo.
046/2016, Afr. Ct. H.P. Rights, ¶¶ 71-78 (2018) (finding child marriage of girls
to constitute impermissible discrimination and harmful practice under the Maputo
Protocol and African Charter on the Rights and Welfare of the Child).
[335] Rebecca J. Cook & Simone
Cusack, Gender Stereotyping: Transnational Legal Perspectives, 9 (2010).
[336] CEDAW Committee, General
Recommendation No. 33 on Women’s Access to Justice, U.N. Doc. CEDAW/C/GC/33
(Aug. 3, 2015) ¶ 26.
[337] X. v. Timor Leste, CEDAW
Committee, U.N. Doc. CEDAW/C/69/D/88/2015 (2018). When sentencing the
complainant, one of the State’s judges told her that the court had decided to
give her a lengthy sentence because “you have taken the life of one of the
nation’s people . . . . As a wife, you must protect your husband.”
See id., ¶¶ 2.15, 6.5.
[338] Marc Bookman, Sex Shamed to
Death: How Oklahoma Prosecutors Used Sex and Infidelity to Put a Woman on Death
Row, The Appeal (2017), available at
https://theappeal.org/sex-shamed-to-death-5a28cc7cf2fc/.
[339] See generally Patricia
Easteal et al.,
How are Women Who Kill Portrayed in Newspaper Media? Connections with social
values and the legal system, Vol. 51 Women’s Studies International Forum 1,
31- 32 (2015), available at
https://www.academia.edu/16739529/How_are_women_who_kill_portrayed_in_newspaper_media_Connections_with_social_values_and_the_legal_system
>; C. Nathan DeWall, T. William Altermatt, & Heather Thompson,
Understanding the Structure of Stereotypes of Women: Virtue and Agency as
Dimensions Distinguishing Female Subgroups, 29 Psychology of Women
Quarterly 4, 396 (2005), available at
http://citeseerx.ist.psu.edu/
viewdoc/download;jsessionid=7879848FE675AF6719190491B42D7432?doi=10.1.1.556.972&rep=rep1&type=pdf
>; Gendered Innovations, Stereotypes, University of Stanford
Gendered Innovations in Science, Health & Medicine, Engineering, &
Environment, available at https://genderedinnovations.stanford.edu/terms/stereotypes.html, last
accessed Sep. 21, 2021.
[340] Patricia Easteal et al.,
How are Women Who Kill Portrayed in Newspaper Media? Connections with social
values and the legal system, 51 Women’s Studies International Forum 1, 32
(2015), available at
https://www.academia.edu/16739529/How_are_women_who_kill_portrayed_in_newspaper_media_Connections_with_social_values_and_the_legal_system
>.
[341] Id.
[342] Id.
[343] See Rachael E. Collins,
‘Beauty and bullets’: A content analysis of female offenders and victims in
four Canadian newspapers, 52 Journal of Sociology 2, 11 (2014), available at
http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.824.2907&rep=rep1&type=pdf
>.
[344] Cf. Elizabeth K. Carll,
News Portrayal of Violence and Women, 46 American Behavioral Scientist,
1601, 1602–1604 (2003), available at
https://de.booksc.eu/book/40322770/2f466d.